Downloaded 257 times



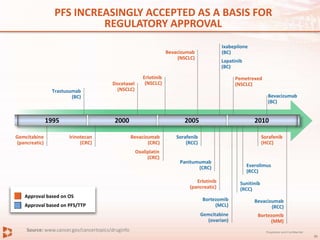
![What are the views of the regulatory agencies
on clinical trial endpoints?
“Acceptable primary endpoints
include OS and PFS/disease free
survival […] While it is generally
acknowledged that the aim of
treatment is to improve quality of life
and survival, restraints on the
conduct of clinical trials may make
these goals unattainable.”
EMA Guideline on the Evaluation of
Anticancer Medicinal Products in Man
“The analysis of OS may be
confounded by crossover and/or
subsequent therapies.
PFS, measured prior to the
introduction of other therapies,
may more accurately depict a
treatment’s therapeutic effect.”
FDA Oncology Head
Richard Pazdur
“PFS can reflect tumour growth and be assessed before the
determination of a survival benefit. Its determination is not
confounded by subsequent therapy.”
FDA Guidance for Industry: Clinical Trial Endpoints for the
Approval of Cancer Drugs and Biologics
EMA Guideline 2009; FDA Guidance For Industry 2009](https://image.slidesharecdn.com/la5egwrtlmeob3gvmqil-signature-ec22a08eed70ccbc104b03b4c3052d6d24d79497c9b73bb439bb3825368824d3-poli-141123211727-conversion-gate01/85/Drug-Purchasing-Pricing-industry-perspective-40-320.jpg)


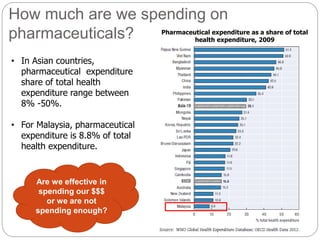
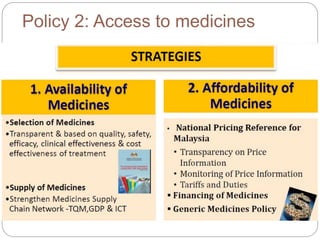
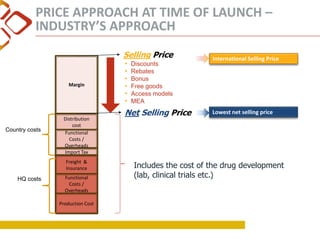
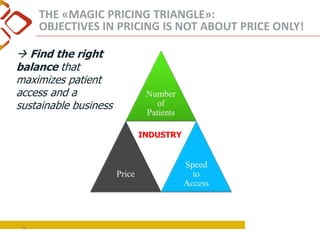
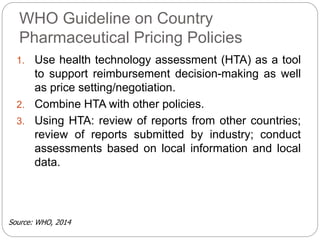
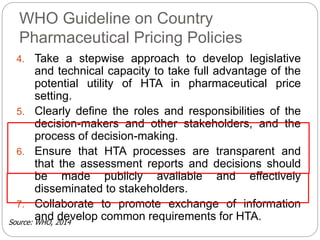
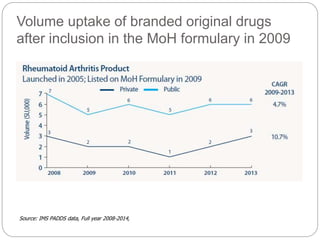
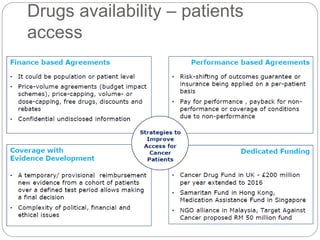
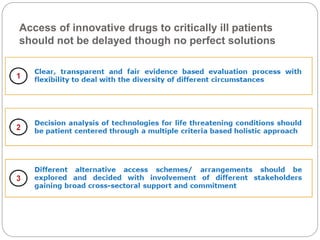
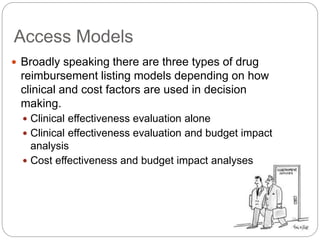
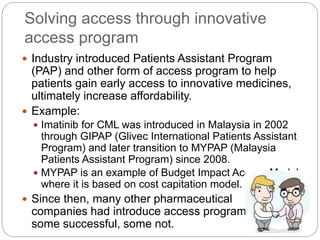
This document summarizes a presentation given by David Lin from Novartis Oncology on drug purchasing and pricing from the pharmaceutical industry perspective. The presentation covers: - The growing demand for healthcare and new treatments putting pressure on pricing and access - Malaysia's national medicine policy and efforts to improve access to medicines through affordability - Factors considered in pharmaceutical pricing like production costs, reference pricing to other countries, and balancing access and sustainability - Efforts by industry like access programs to help patients gain early access to innovative treatments - The changing treatment landscape with new cellular and personalized therapies requiring new frameworks for evaluation and pricing assessment.



![Abbreviated New Drug Application [ANDA]](https://cdn.slidesharecdn.com/ss_thumbnails/abbreviatednewdrugapplicationanda-160619062810-thumbnail.jpg?width=640&height=640&fit=bounds)
![Investigational New drug application [INDA]](https://cdn.slidesharecdn.com/ss_thumbnails/investigationalnewdrugapplicationinda-160619063044-thumbnail.jpg?width=640&height=640&fit=bounds)


























































































