Downloaded 1,181 times





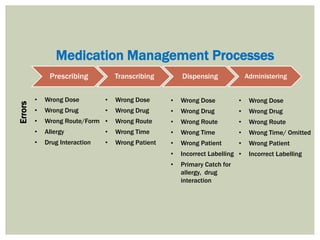

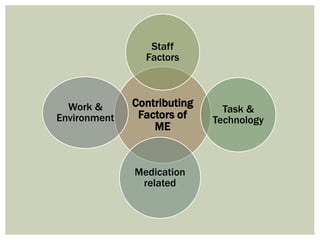

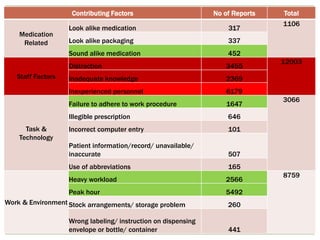
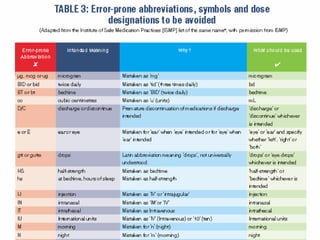
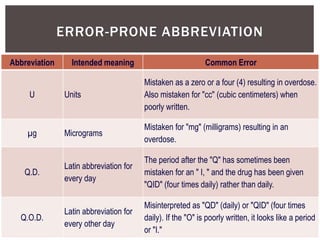
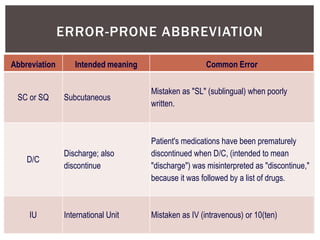
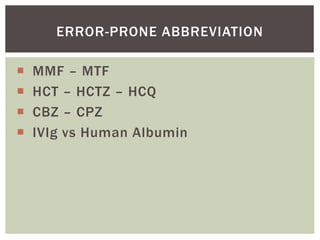
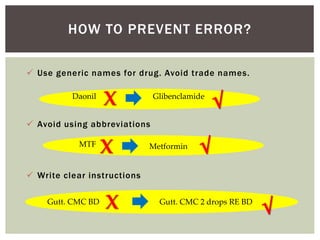
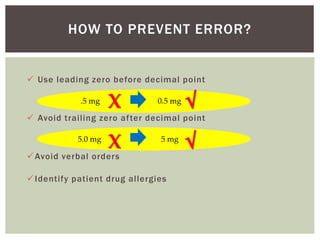



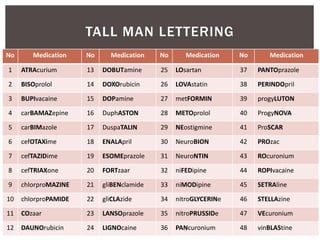
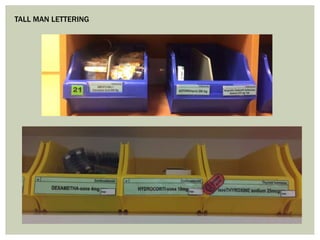




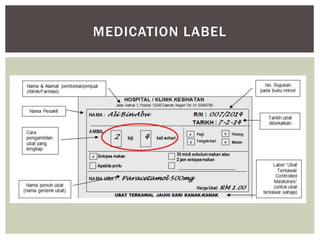

The document describes a case of medication error where a patient was wrongly administered pancuronium instead of an antacid, causing respiratory arrest. It provides definitions of medication error and discusses the prevalence and impact of medication errors. It identifies common types of errors like wrong dose, wrong drug or wrong route. Contributing factors discussed include look-alike packaging, sound-alike names, distractions, workload and abbreviations. Strategies to prevent errors include separating high-alert medications, tall man lettering, double checks and education.





















































































