Downloaded 101 times
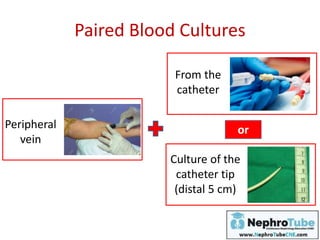
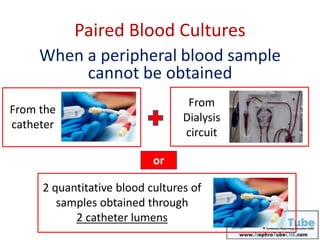
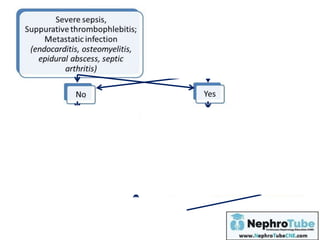
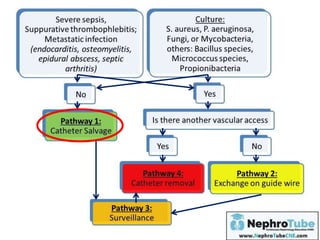
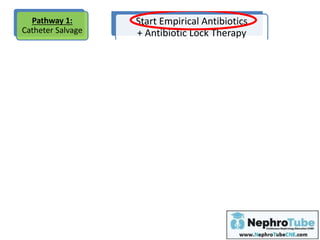

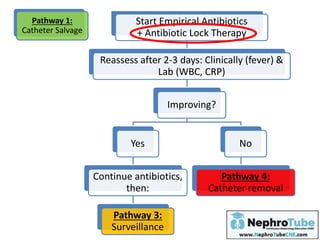
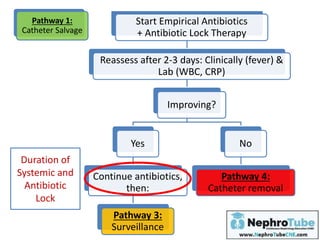
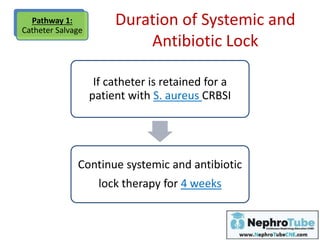
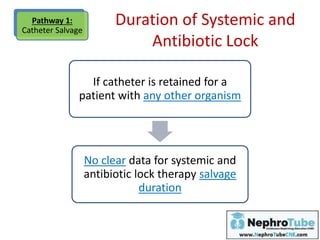
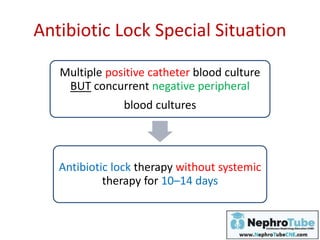
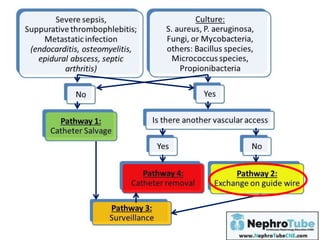
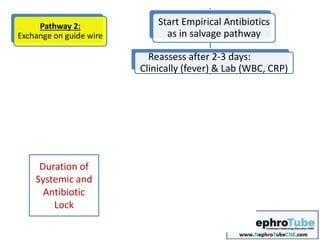
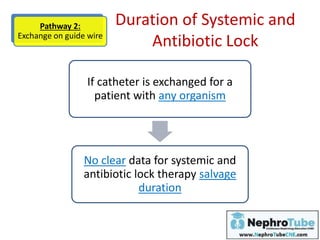
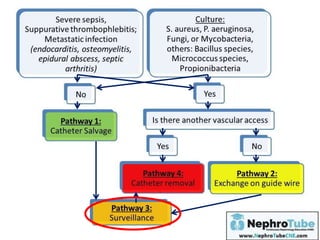
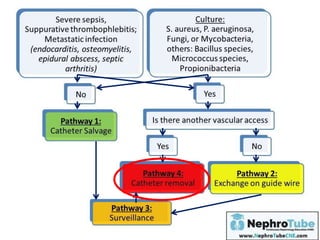
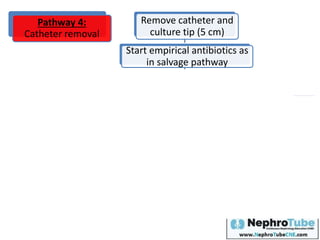
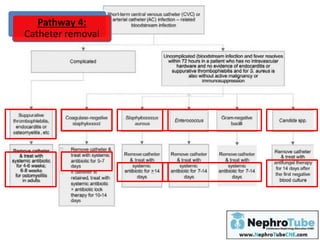

This document discusses the diagnosis and management of catheter-related bloodstream infections (CRBSI) in hemodialysis patients. It outlines the following key points: 1. CRBSI can be diagnosed through paired blood cultures, with the same organism growing in both indicating infection. Catheter tip cultures can also help diagnose CRBSI. 2. Management involves starting empirical antibiotics and antibiotic lock therapy, then assessing response and either continuing treatment, exchanging the catheter, or removing it depending on improvement. 3. Prevention strategies include using aseptic technique during catheter insertion and care, avoiding non-tunneled and femoral catheters when possible, monitoring exit sites, and considering antimicrobial lock therapy or













































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)









