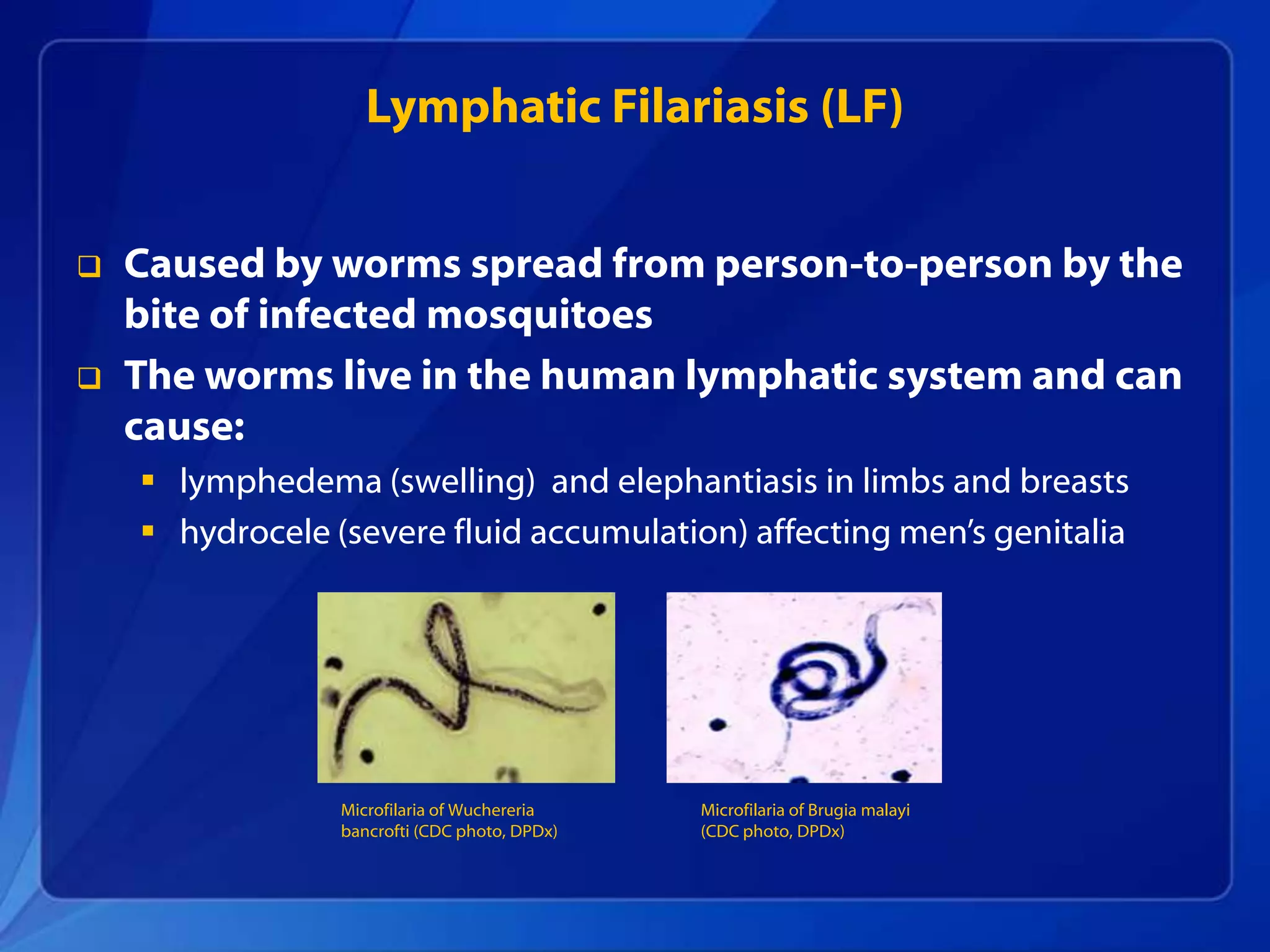
Lymphatic filariasis is a disabling tropical disease spread by mosquitoes that causes swelling of the limbs and genitals. It impacts over 120 million people worldwide and is targeted for global elimination by 2020. Mass drug administration of medications that interrupt transmission has protected millions from infection and been delivered to over 2.8 billion people across 53 countries with support from the CDC and partners. While transmission continues in some parts of the Americas, regional elimination is achievable with sustained control efforts such as expanding treatment coverage and improving disease management.