- Documentation refers to written evidence of interactions between healthcare professionals, patients, and families regarding treatments, procedures, and patient responses.
- The major purpose of medical documentation is to record the care provided to the patient and allow for continuity of care between professionals. It also serves as a legal document.
- Inadequate documentation can be a nurse's worst legal liability, while well-documented records provide the greatest legal protection. Documentation must clearly depict the complete picture of care provided and ensure it meets standards.




























































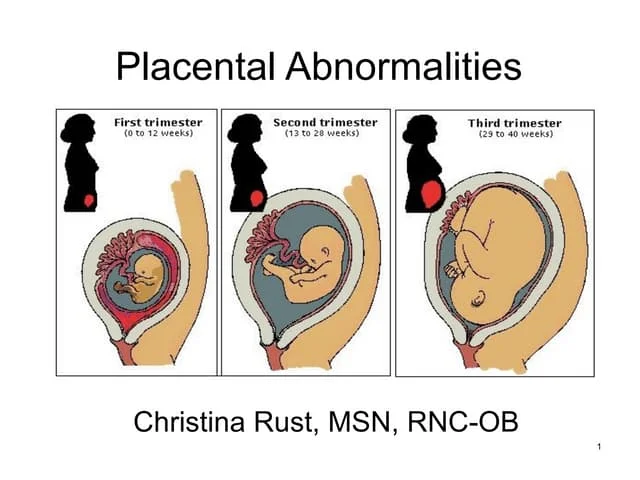















![H:\Abnormal Implanataion[1]](https://cdn.slidesharecdn.com/ss_thumbnails/habnormalimplanataion1-100305152320-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)
![H:\Physiological Changes In Pregnancy[2]](https://cdn.slidesharecdn.com/ss_thumbnails/hphysiologicalchangesinpregnancy2-100305140624-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)



















