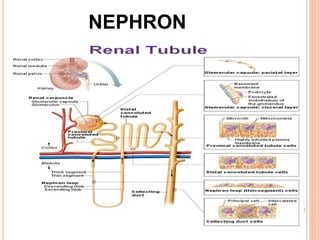
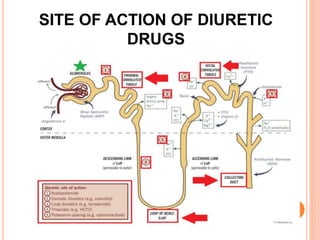
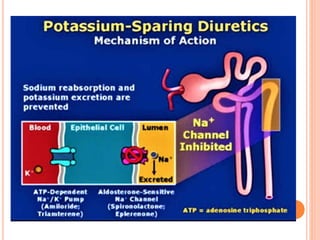
Diuretics are drugs that promote the loss of sodium and water through urine, categorized into high, medium, and low efficacy types. They work by inhibiting various mechanisms in the nephron, particularly in areas such as the ascending loop of Henle and distal tubule, and are used to treat conditions like heart failure, hypertension, and edema. Side effects include electrolyte imbalances and volume depletion, depending on the specific class of diuretic used.