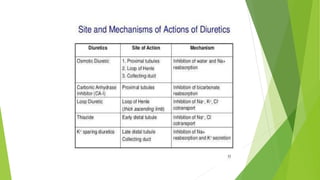
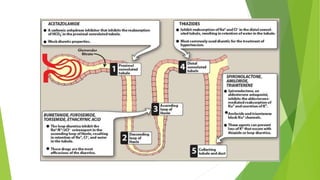
Diuretics work by interfering with electrolyte reabsorption in the kidney to promote excretion of sodium and water. They are classified based on where in the nephron they act: carbonic anhydrase inhibitors act in the proximal convoluted tubule; loop diuretics act on the ascending loop of Henle; thiazide diuretics act in the distal convoluted tubule; and aldosterone inhibitors act on the collecting tubule. Common diuretics include acetazolamide, furosemide, hydrochlorothiazide, and spironolactone. They are used to treat conditions like hypertension, heart failure, and edema. Adverse effects can include electrolyte imbalances like hyp