Download to read offline

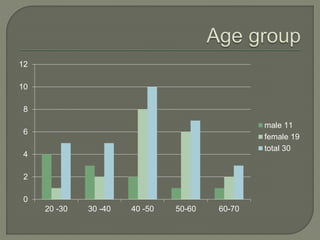
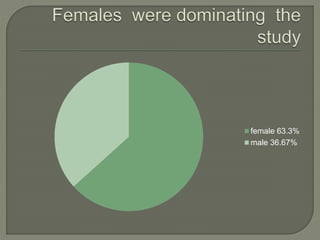
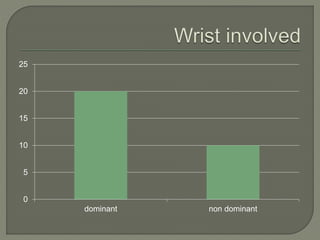
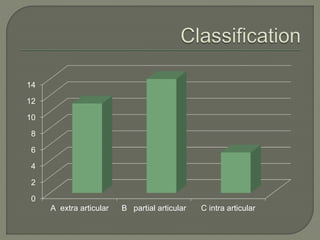
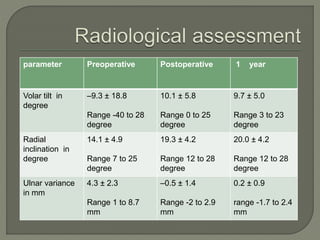
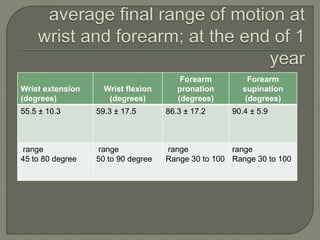
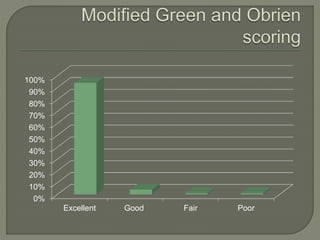


This study evaluated the functional outcomes of using volar plating to surgically treat fractures of the distal radius. 30 patients underwent open reduction and internal fixation with a volar plate. At one year follow up, wrist range of motion, grip strength, and alignment had significantly improved. Nearly 90% of patients reported excellent or good results based on the Modified Green and O'Brien scoring system. While a few patients developed minor complications like tenosynovitis, no patients had non-union or implant failures. Overall, volar plating provided an effective treatment that led to high levels of patient satisfaction through restored wrist function and limited pain.




























![www corrected shahab '24 JC Colle's fracture [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/wwwcorrectedshahab24jccollesfractureautosaved-250519081914-6e733621-thumbnail.jpg?width=640&height=640&fit=bounds)
![shahab '24 JC Colle's fracture [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/shahab24jccollesfractureautosaved-250519081834-ced3d7e8-thumbnail.jpg?width=640&height=640&fit=bounds)
























![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)


![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)





![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)


