MANAGEMENT OF DORSALLYDISPLACED
INTRAARTICULAR FRACTURE OF THE
DISTAL RADIUS WITH DORSAL LOCKING
PLATE
PRESENTER: DR PRAVIN TODEKAR 3RD
YEAR PGT
PROF SANJIB WAIKHOM
HOD DEPT OF ORTHOPAEDICS
RIMS, IMPHAL
2.
Distal radius fracturesaccount for 17% of all fractures treated by
orthopedic trauma surgeons, with 60% being intra-articular and unstable.
The primary goal of treatment is precise reduction and stable fixation.
Treatment options include casting, percutaneous pinning, ligamentotaxis
and open reduction and fixation with volar or dorsal plating.
INTRODUCTION
3.
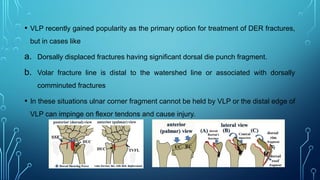
• VLP recentlygained popularity as the primary option for treatment of DER fractures,
but in cases like
a. Dorsally displaced fractures having significant dorsal die punch fragment.
b. Volar fracture line is distal to the watershed line or associated with dorsally
comminuted fractures
• In these situations ulnar corner fragment cannot be held by VLP or the distal edge of
VLP can impinge on flexor tendons and cause injury.
4.
• Advantages ofdorsal plating
a. Direct visualization of articular surface.
b. Provides a buttress against dorsal collapse.
c. Lowers the risk of neurovascular structure damage.
• Dorsal plate has higher incidence of tendon complications but the newer
generation low profile plates overcome these complications.
5.
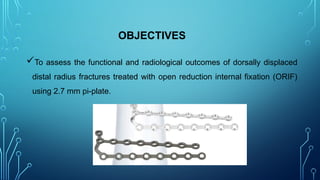
OBJECTIVES
To assess thefunctional and radiological outcomes of dorsally displaced
distal radius fractures treated with open reduction internal fixation (ORIF)
using 2.7 mm pi-plate.
6.
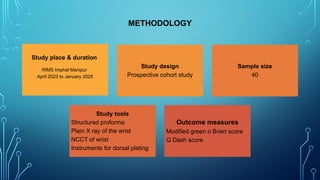
Study place &duration
RIMS Imphal Manipur
April 2023 to January 2025
Study design
Prospective cohort study
Sample size
40
Study tools
Structured proforma
Plain X ray of the wrist
NCCT of wrist
Instruments for dorsal plating
Outcome measures
Modified green o Brien score
Q Dash score
METHODOLOGY
7.
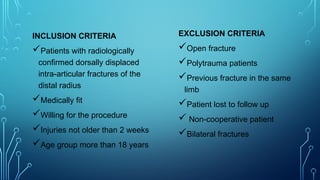
INCLUSION CRITERIA
Patients withradiologically
confirmed dorsally displaced
intra-articular fractures of the
distal radius
Medically fit
Willing for the procedure
Injuries not older than 2 weeks
Age group more than 18 years
EXCLUSION CRITERIA
Open fracture
Polytrauma patients
Previous fracture in the same
limb
Patient lost to follow up
Non-cooperative patient
Bilateral fractures
Subperiosteal elevation of
4th
and2nd
extensor
compartment and fracture
site exposed
Dorsal plate (Pi plate) fixed
over fracture fragments
Retinaculum is closed and
EPL kept superficial to it
Sutured wound
POSTOPERATIVE FOLLOW-UP
Rom exercisestarted on the 3rd
post-op day.
Patients were followed up on 12th
day, at 6 weeks, 12 weeks, 24 weeks and after
1 year.
Sutures removed on 12th
day.
During each visit radiographic parameters and functional outcome (Q DASH &
Modified green O’Brien score) were assessed.
17.
RESULTS
DEMOGRAPHICS
This study included40 patients
Aged between 20 to 50 years
Male to female ratio of 3:1
Mean duration of follow-up is 24 weeks, and mean fracture union time is 6
to 8 weeks
The most common mode of injury is RTA (56%) followed by FOOSH (28%)
followed by fall from height (12%), and others (4%).
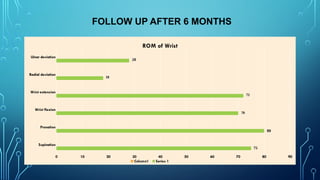
FOLLOW UP AFTER6 MONTHS
Supination
Pronation
Wrist flexion
Wrist extension
Radial deviation
Ulnar deviation
0 10 20 30 40 50 60 70 80 90
ROM of Wrist
Column1 Series 1
75
80
70
72
18
28
20.
The functional outcomeof participants was assessed using Q DASH
score and Modified Green O’Briens score at various follow-up intervals
According to the Q DASH score 32 patients had an excellent outcome, 7
patients had a good outcome and 1 patient had a fair outcome.
According to Modified Green O’Briens score 29 patients had an excellent
outcome, 10 patients had good outcome and 1 patient had poor outcome.
21.
COMPLICATIONS
There were noplate breakage, infections, tendon rupture, or
compression neuropathy during the study period
Tendon irritation was observed in one patient for which plate removal
was done after 6 months.
22.
CONCLUSION
Dorsal locking plateis a useful technique for the treatment of selected
cases of dorsally displaced, comminuted intra-articular fractures of the
distal radius.
Tendon complications can be avoided by careful subperiosteal elevation
of 2nd
and 4th
compartment and avoiding direct contact of plate with a
tendon.










![shahab '24 JC Colle's fracture [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/shahab24jccollesfractureautosaved-250519081834-ced3d7e8-thumbnail.jpg?width=640&height=640&fit=bounds)

![www corrected shahab '24 JC Colle's fracture [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/wwwcorrectedshahab24jccollesfractureautosaved-250519081914-6e733621-thumbnail.jpg?width=640&height=640&fit=bounds)











































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)