Introduction:
DVD is aform of vertical deviation that is basically
characterized by:
a hyperdeviation in one eye that is present while the other
eye is fixing with the non-fixing eye slightly exorted and
abducted,
no hypodeviation is seen when the fixation is changed to
the other eye which differentiates DVD from other typical
vertical deviation
3.
• Other termsfor DVD are: anatopia, alternating
hyperphoria / hypertropia, alternating sunsumduction,
dissociation double hypertropia, dissociated vertical
divergence, occlusion hyperphoria / tropia
• B/L hyperdeviation is seen which is usually asymmetrical
with longer component a/w non-dominant eye
• Since the upward drifting of the non-fixing eye is often a/w
abduction & excyclotorsion, the term "Dissociated
Strabismus Complex" (DSC) has been denoted for DVD, DHD
& DTD
4.
Etiology:
1)Bielchowsky's theory ofpositive and negative sub-cortical
vertical divergence centers: He theorized that DVD occur due
to alternating & intermittent excitation of both sub-cortical
divergence centers
2) Theory of imbalance binocular stimulation: Spielman
postulated that DVD may be caused by imbalance of
binocular stimulation due to its frequent a/w infantile
esotropia & sensory heterotropia
3)Brodsky theory: Accdn to this theory, DVD is a vestigial
remnant of dorsal light reflex
5.
Etiology:
Others:
Elastic preponderanceof the elevators & depressors (esp.
lateral paresis of depressor)
Imbalances between the amount of innervation originating
from vestibular organ
Undesirable byproduct of "Nystagmus Damping
Mechanism"
Monocular conjugate mechanism plus a binocular
mechanism
Theory of defective monocular nasal retinal quadrant stimuli
6.
Clinical features:
Deviation:
Spontaneous occurrence of vertical deviation in either eye
characterized by slow upward drifting of the non-fixing eye.
The vertically deviated eye is also extorted and slightly
abducted
Association of DVD:
Essential infantile esotropia (75%), infantile exotropia,
sensory heterotropia , A- pattern exotropia, excycloduction of
the elevated eye & latent nystagmus, incycloduction of fixing
eye
7.
Clinical features:
Headposture:
Approx. 1/3rd of the pt with DVD have AHP in which head is
tilted away from deviating eye, & chin depression
Laterality:
DVD is frequently B/L (alternating sursumduction) but rarely
may be monocular
8.
Clinical features:
Binocularvision & sensory adaptation:
-Suppression usually develops in patients with spontaneous
DVD &
thus eliminates diplopia
-Peripheral fusion is often present in patient with DVD having
a
manifest deviation of 4Δ or less
-Absolute facultative central scotoma in one eye, while both
eye are being used for peripheral vision
9.
Clinical features:
Symmetry:
UsuallyB/L & asymmetrical
Bielchowsky phenomenon:
On decreasing the visual input to fixing eye by holding filters
of increasing density, efforts to maintain fixation triggers
abnormal innervation to the elevators which inturn elicits a
compensatory innervation to the depressor
Monocular DVD:
• Monoculardissociated hyperdeviation may be seen in
presence of IXT
• Found when fusion is broken, deviated eye develops small
hyperdeviation
• Deviation is not a/w yoke muscle & is absent when
deviated eye is not in abduction
• Generally disappears following horizontal sx correction
12.
Binocular DVD: (Alternating
sursumduction)
•Either eye elevates under cover (double hyperdeviation)
along with slight extorsion & abduction
• On removal of cover, eyes slowly depress & intort
• No corresponding hypotropia of fellow eye
13.
Diagnosis:
1)Cover-Uncover test:
In ptwith U/L manifest DVD, covering the fixing eye
causes downward movement of uncovered eye
In pt with alternate DVD, covering either eyes elevate
them while uncovered eye moves downward to take
fixation
In pt with latent DVD, no movement of the uncovered eye,
eye under cover is elevated & moves downward after it is
covered. DVD is present only when eyes have been
dissociated
14.
Diagnosis:
2)Head tilt test:
IncreasedDVD on contralateral head tilt
Few pt. show converse response
3)Red-glass test:
Diplopia can be elicited in most pt. with dark red glass
The fact that pt. will localize the red image below the
fixation light, regardless of whether the red glass is held
before right or left eye clearly differentiates DVD from
other vertical deviation
15.
Diagnosis:
4) Demonstration ofBielchowsky's phenomenon
5) Measurement of deviation:
I) Prism base down is placed in front of the deviating eye
under occlusion to measure the hyperdeviation. ACT is
performed until no downward movement of the eye is seen
II) Modified Krimsky
III) Grading: 1+: a slight deviation
2+: a small deviation
3+: moderate deviation
4+: large deviation
A) Non-surgical treatment:
•Not very effective
• Conservative therapy in the form of changing the
fixation pattern by patching or optical means
• Indicated in pts with asymmetric involvement
18.
B) Surgical treatment:
•Indications: -Large manifest DVD
-Significant AHP
• Techniques: -Faden operation with SR recession
-Large recession of SR
-Resection of IR
-Recess-resect procedure
-Recession of IO with anteriorization of
its
insertion
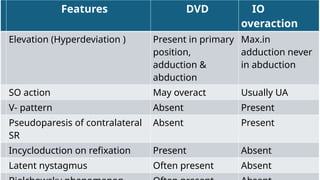
Features DVD IO
overaction
Elevation(Hyperdeviation ) Present in primary
position,
adduction &
abduction
Max.in
adduction never
in abduction
SO action May overact Usually UA
V- pattern Absent Present
Pseudoparesis of contralateral
SR
Absent Present
Incycloduction on refixation Present Absent
Latent nystagmus Often present Absent