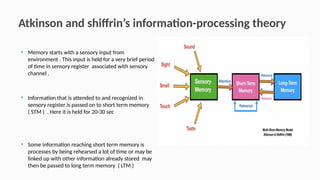
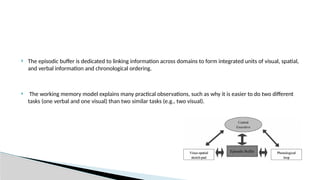
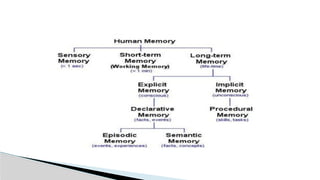
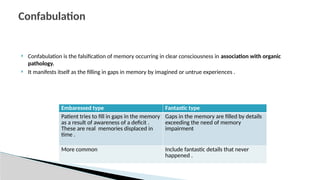
This document discusses memory disorders and the processes of memory storage, retrieval, and forgetting. It outlines models of memory, including the working memory model by Baddeley and Hitch, types of memory such as explicit and implicit memory, as well as various amnesias and distortions of memory. Clinical classifications and testing methods for assessing memory capabilities are also explored.