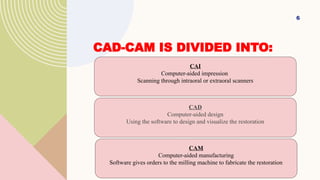
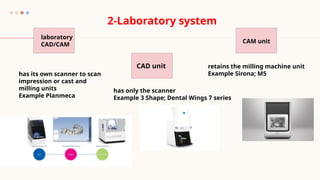
The document discusses the evolution and advantages of digital impressions and CAD/CAM technologies in dentistry, highlighting systems like CEREC for real-time restoration processes. It outlines both benefits, such as patient satisfaction and efficiency, and drawbacks, including high initial costs and scanning limitations. Additionally, it details intraoral and extraoral scanning methods, data acquisition processes, and potential errors during scanning.