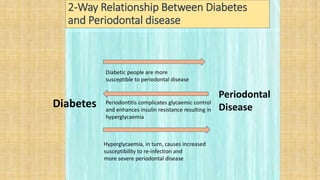
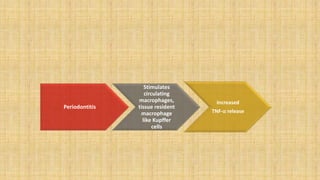
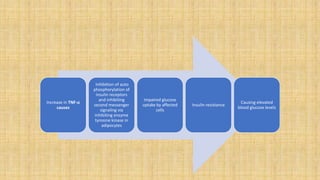
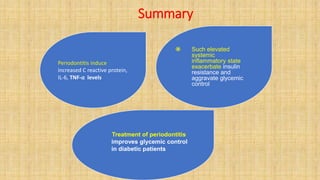
The document discusses the bidirectional relationship between diabetes and periodontitis, highlighting that patients with diabetes are more prone to periodontal disease and that periodontitis can complicate glycemic control, leading to more severe diabetes symptoms. It details the pathological mechanisms involved, the implications for treatment in uncontrolled diabetes, and how effective periodontal therapy can improve glycemic control in diabetic patients. Additionally, it emphasizes the importance of meticulous oral hygiene and supportive therapy to manage both conditions.