Download to read offline
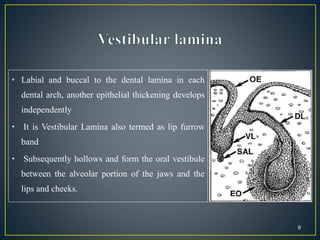

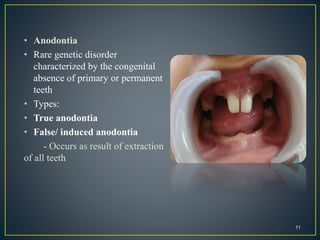
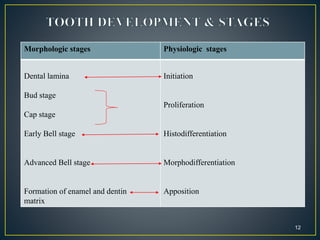
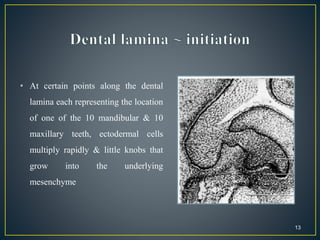

























This document summarizes the process of tooth development from the dental lamina through the various stages to clinical considerations. It begins with the dental lamina and vestibular lamina developing from the oral ectoderm. Tooth buds then develop from the dental lamina, going through the bud, cap and bell stages as the enamel organ, dental papilla and follicle form. Root development occurs after crown formation. The stages and common anomalies in tooth development are described to provide dentists with an understanding of this complex process.















































































