MORPHOLOGY
Refers to Generalappearance of skin lesions irrespective of etiology.
• Location/ symmetry / distribution / site
• Colour
• Surface/ texture
• Pattern of lesions
• Consistency
• Demarcation of margins
• Freely mobile/attached to underlying tissue
3.
DISTRIBUTION
• Symmetrical –Psoriasis affects the elbows and knees
-Dermatitis herpetiformis
-Syringomas -the lower lids.
• Flexural – flexural psoriasis
Atopic eczema- flexures - antecubital & popliteal
Fossae.
benign familial pemphigus -axillae and groins
• Dermatomal/zosteriform- Along single spinal aff. Nerve
4.
• Lymphangitic-implies aninfectious agent that is spreading centrally from an acral site,
red streak along limb
-Staphylococcal/ streptococcal cellulitis.
• Acral: Occurring in distal locations, such as on the hands, feet, wrists, and ankles -
palmoplantar pustulosis, chilblains
• Intertriginous: Occurring in the skin folds - axillae, inguinal folds, inner thighs,
inframammary skin, related to moisture and heat generated in these areas- candidiasis
• Generalized: Widespread.
consisting of inflammatory (red) lesions -called an exanthema (rash), macular, papular,
vesicular- viral exanthems, drug eruption
• Universal: Involving the entire cutaneous surface - erythroderma, alopecia universalis
Erythroderma – this is defined as generalized redness often with scaling, affecting
90% of the skin surface. It may be a primary skin disease such as psoriasis, atopic or
seborrhoeic eczema, drug induced, congenital (such as in the ichthyosiform
erythrodermas), due to T cell lymphoma of the skin or idiopathic.
‐
5.
• Sun exposed:–dermatoses caused by light occurring in
areas not covered by clothings- face, bald scalp, ‘V’ area of the
chest and the backs of the hands with a cut off at the point
‐
where sleeves cover the skin.
-chronic actinic dermatitis,photodermatitis, subacute cutaneous
lupus erythematosus, polymorphous light eruption, squamous
cell carcinoma)
• Sun protected: Occurring in areas covered by one or more
layers of clothing,dermatosis improved by sun exposure —
parapsoriasis, mycosis fungoides
• Airborne – this includes the face and hands, similar to photo
distribution but the light shaded sites of the upper lid,
‐
Wilkinson’s triangle and finger webs are affected.
Allergens include plants, epoxy resins, phosphorus sesquisulfide
(the red tip match allergen) and wood dusts.
6.
PATTERN / ARRANGEMENT
•Agminate – clustered;
acne agminata
agminate naevi, clustering of melanocytic naevi.
• Grouped/ herpetiform – lesions clustered together
characteristic of some infections- herpetic vesicles, molluscum
contagiosum, plane warts
-flea bites,
-endogenous lesions such as lichen planus, lymphangioma
circumscriptum.
• Satellite – a cluster of lesions around a larger central lesion.
• Confluent – lesions merging together, locally or widespread-
pityriasis versicolor.
7.
TYPE
• PRIMARY- nativeappearance of skin lesions
• SECONDARY- reflect the effects of exogenous factors or temporal changes that
evolves during the course of skin disease
• SPECIAL
MACULE
• Flat
• Circumscribed
•Non palpable
• Size < 1cm
• Differs in colour from surrounding skin
PATCH
• Flat
• Circumscribed
• Non palpable
• > 1 cm
10.
PAPULE
• Elevated
• Solid
•< 1cm
• Above the plane of surrounding skin
• Can be sessile, pedunculated,flat
topped,umblicated,verrucous
• Hyperplasia of epidermal, dermal
components.
Flat topped, glistening surface – LP. papules of common warts
11.
NODULE
• Solid, round/ellipsoid
• Elevated,
• depth differentiates nodule and papule
• Palpable
• > 1cm
• Nodules can be due to inflammation, metabolic
deposits, or neoplasms.
• Epidermal nodules -nodular basal cell carcinoma
and keratoacanthoma.
• Dermal nodules-Metastatic carcinoma,
lymphomas, histoid leprosy and
dermatofibromas Dermatofibroma Erythematous elevated
subcutaneous nodules in EN
12.
• Subcutaneous nodules-Lipomas,tendinous
xanthomas, and erythema nodosum
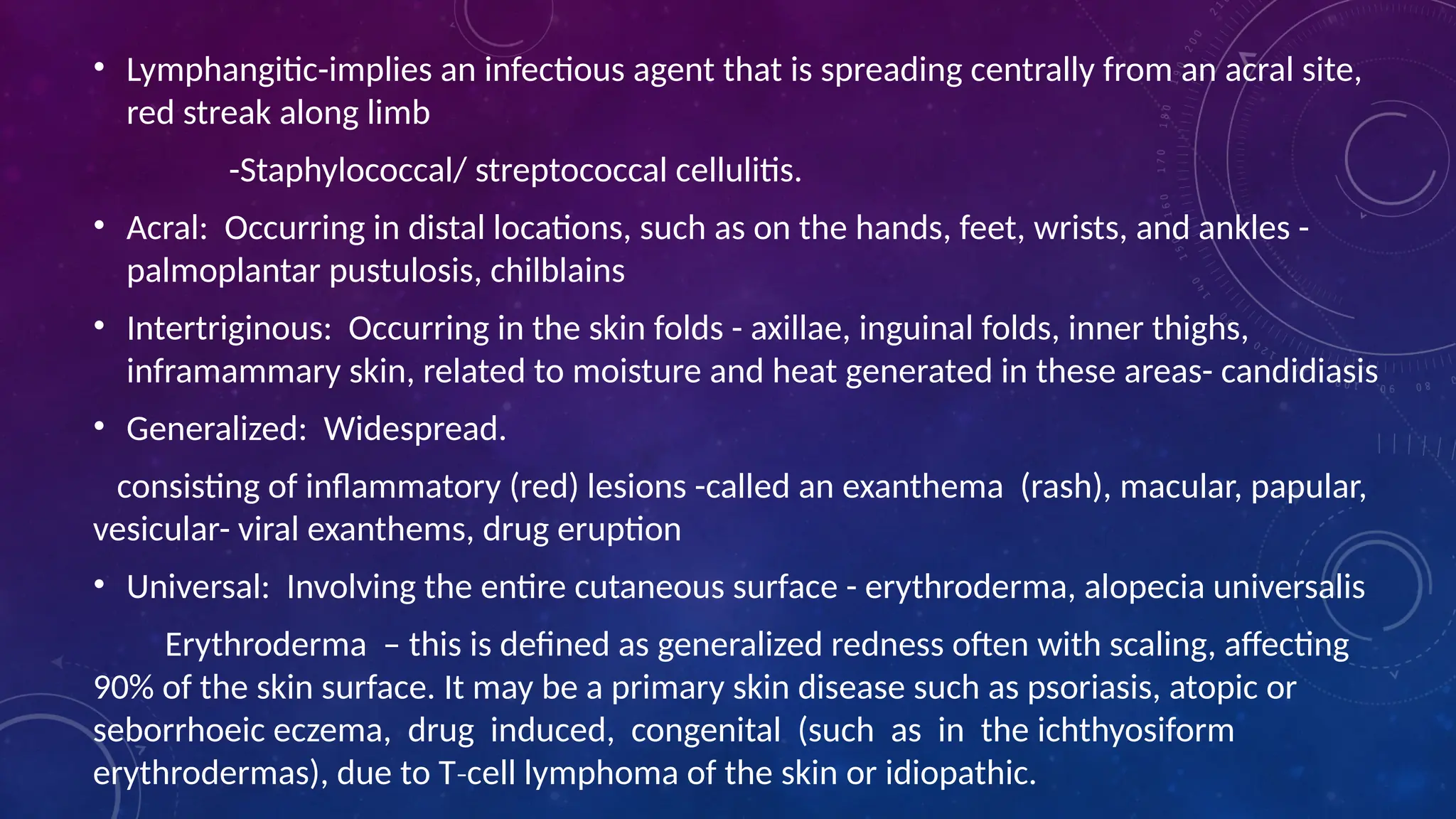
• Surface of the nodule could be ulcerated,
fungating, smooth, or keratotic.
• Gumma-specifically used for the granulomatous
nodular lesion of tertiary syphilis.
• Tumor, also sometimes included under the
heading of nodule, is a general term for any
mass, benign or malignant.
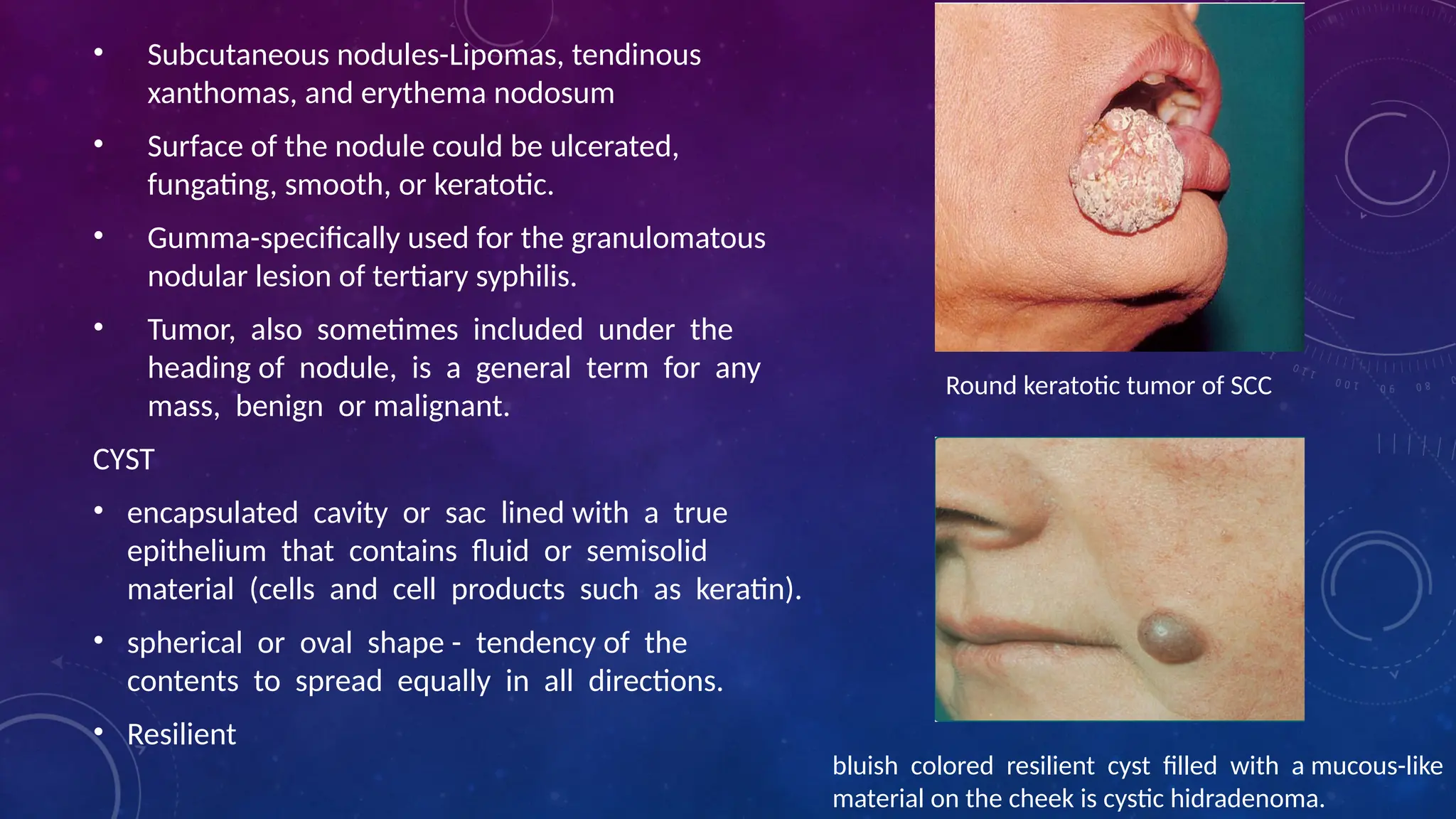
CYST
• encapsulated cavity or sac lined with a true
epithelium that contains fluid or semisolid
material (cells and cell products such as keratin).
• spherical or oval shape - tendency of the
contents to spread equally in all directions.
• Resilient
bluish colored resilient cyst filled with a mucous-like
material on the cheek is cystic hidradenoma.
Round keratotic tumor of SCC
13.
PLAQUE
• Plateau likeelevation
• Circumscribed
• > 1cm
• Enlargement of papule / coalescing of papules
Atrophic depigmented plaque of dle
14.
Vesicle
• Circumscribed
• Elevated
•Filled with fluid- clear, serous, hemorrhagic
• < 1cm
• Lesions may be tense (bullous pemphigoid),
flaccid ( pemphigus)
umbilicated – collapsed centre (varicella)
PUSTULE
• Circumscribed
• Elevatedcavity in epidermis/ infundibulum
• Purulent material- leukocytes with/without
cellular debris, bacteria/ sterile, white, yellow,
or greenish-yellow
FURUNCLE
• deep necrotizing folliculitis with
suppuration. inflamed follicle-centered
nodule usually greater than 1 cm with a
central necrotic plug and an overlying
pustule.
• Several furuncles may coalesce to form a
carbuncle.
17.
WHEAL
• Transient elevation
•Dermal/ hypo dermal edema
• Pale centrally with erythematous rim
• Borders sharp but unstable ,may be tiny papules or
giant plaques, and they may take the form of various
shapes (round, oval, serpiginous, or annular)
• Transient vascular reaction in the upper dermis in which
there is both vasodilation and increased permeability of
the capillaries giving rise to edema.
• The epidermis is unaffected and there is no scaling
• Stroking of normal skin may produce wheals-
Dermatographism.
• Angioedema -diffuse, deep, edematous reaction
occurring in areas with loose dermis and subcutaneous
tissue such as the lip, penis, and hands and the larynx
(which may be fatal because of obstruction).
18.
SECONDARY
• Crust- driedserum/ other exudates with
disruption of skin surface.(serum, blood,
or purulent exudate)
yellow-brown when formed from dried
serous secretion
turbid yellowish-green when formed
from purulent secretion
reddish-black when formed from
hemorrhagic secretion.
When blood forms a major component of
the crust, it is often referred to as a scab.
19.
• Fissure- lineargap/ slit in skin surface from
excessive tension or decreased elasticity of the
involved tissue.
Palm and soles as st. Corneum is least
expandable here.
• Excoriation- loss of skin substance esp due to
scratching
• Erosion-
moist,circumscribed,depressed, superficial,
erythematous, and covered with serous exudate.
loss of epidermis heals without scarring,
20.
• ULCER
loss ofepidermis and dermis(upper)
often with underlying tissue.
Heals with scarring
Borders- rolled, undermined, punched
out, jagged, or angular.
base - clean, ragged, or necrotic.
Discharge - purulent, granular, or
malodorous.
Surrounding skin may be red, purple,
pigmented, reticulated, indurated,
sclerotic, or infarcted
• Lichenification-thickening of epidermis
in response to prolonged rubbing (tree
bark) with accentuating of skin
markings.
ragged base and heaped-up pink
erythematous border -progressing
pyoderma gangrenosum.
21.
SCALE
Scale- flat plate/flake of St. corneum, formed
when there is either an excess production or
increased adherence of the cells of the
stratum corneum (preventing the normal
dislodging of individual cells)
When scaling papules are the predominant
feature of a disease, the eruption is described
as papulosquamous. Fine scales occur in the
macular lesions of tinea versicolor and
erythrasma. These lesions are described as
maculosquamous.
23.
SCAR
• Proliferation offibrous tissue that
replaces previously normal
collagen after a wound or
ulceration breaches the reticular
dermis leading to visible alteration in
the appearance of the skin.
• Scars may be hypertrophic –
papules, plaques, nodules
Atrophic- thin, depressed
• epidermis is thin and devoid of
normal skin marking and
appendages
26.
ATROPHY
• Reduction inthe components of a tissue, organ, or part
of the body.
• May involve the epidermis, dermis, or subcutis
• Epidermal atrophy results from a decrease in the
number of epidermal cells, causing a thinning of the
epidermis, becomes transparent/glossy,the normal skin
lines are lost, and a fine wrinkling (cigarette paper)
• Dermal atrophy results in clinically detectable
depression of the skin.
decrease in the papillary or reticular dermal connective
tissue
without epidermal involvement, skin color and
markings remain normal in the affected area.
Panniculus-more substantial depression.
27.
SPECIAL LESIONS
BURROW
• wavy,threadlike tunnel through the outer portion
of the epidermis excavated by a parasite.
• Scabies mite
• 5 mm in length, on the fingers, wrist, or genitalia
• Longer burrows (5–10 cm) on the feet are seen in
creeping eruption (larva migrans) caused by migration
of hookworm larvae.
MILIUM
• Milia are small, superficial cysts with an epidermal
lining.
• They occur on the face, especially in the periorbital
region
28.
COMEDO
• hair follicleinfundibulum dilated
and plugged by keratin and lipids.
• Open/ black heads-the
pilosebaceous unit is open to the
surface of the skin with a visible
keratinaceous plug,
Black colour -due to the oxidized
sebaceous content of the
infundibulum .
• Closed/White heads-follicular
opening is unapparent.
The lesions appear as tiny papules
somewhat lighter in color than the
surrounding skin
29.
TELENGIECTASIS
• These aredistinctly visible dilated capillaries
• Types- Mat, punctate,stellate, linear
• Poikiloderma refers to a combination of reticulate
telangiectasia, pigmentation, atrophy and
depigmentation
TARGET (iris) LESION-
• These are less than 3 cm in diameter
• Pathognomic of erythema multiforme
• Extremities, especially hands.
• Three zones of colour change are present—
• a central, dark, sometimes blistered, area
• surrounded by a pale edematous zone,
• which in turn is rimmed by another zone of
erythema
30.
PRUPURA
• Extravasation ofred blood from cutaneous
vessels into skin or mucous membranes
resulting in reddish-purple lesions
• Petechiae are small, pinpoint purpuric macules.
• Ecchymoses are larger, bruise-like purpuric
patches.(more than 2 mm)
• Non inflammatory extravasation of blood
• Palpable purpura-suggestion of an
inflammatory insult to the vessel wall as a
cause of extravasation of blood and
inflammatory cells Non blanching red erythematous papules
and plaques (palpable purpura) on the
legs, representing leukocytoclastic vasculitis
Blanchable pink to red color of skin or mucous membrane
that is due to dilatation of arteries and veins in the
papillary and reticular dermis
ERYTHEMA
31.
CONFIGURATION/ SHAPE
• Discoid-(nummular)- filled circle. Discoid eczema, psoriasis
• Petaloid- Discoid lesions which have merged together. Seborrhoeic dermatitis on the trunk
• Arcuate-Incomplete circles. Urticaria
• Annular-Open circles with different central skin compared with the rim. Tinea corporis, granuloma annulare
• Polycyclic-Circles which have merged together. Psoriasis
• Livedo- Chicken wire criss cross pattern. Erythema ab igne, polyarteritis
‐ ‐
• nodosa, microvascular occlusion d/o
• Reticulate Fine lace like pattern Oral lichen planus
‐
• Blood vessels-Thrombophlebitis,
Mondordisease (linear
thrombophlebitis on the
trunk)Eczema related to varicose
veins
• Lymphatics-Lymphangitis,
Sporotrichosis, fish tank granulomas
• Dermatome-Herpes zoster,
zosteriform naevus, zosteriform
Darier disease, zosteriform
metastases
• Nerve trunks-Leprosy (thickened
cutaneous nerves)
• Developmental, Blaschko lines-lines
of skin cell migration during
embryogenesis; generally
longitudinally oriented on the limbs
and circumferential on the trunk.
LINEAR
Lichen striatus
35.
linea nigra,Epidermal naevi,incontinentia pigmenti,
hypomelanosis of Ito,Linear psoriasis, linear lichen planus,
lichen striatus, atrophoderma of Conradi–Hunnerman
disease
• Skin stretching-Striae due to growth spurt (on lower back)
• Infestation-Scabies, larva migrans (both usually serpiginous)
• Physical-
Trauma to previously normal skin-Keloid scar, bruising,
dermatitis artefacta, amniotic constriction bands
Trauma to skin with a pre existing dermatosis-Purpura
‐
(cryoglobulinaemia, amyloid, vasculitis)Blisters (epidermolysis
bullosa, porphyrias)
Koebner phenomenon
• External agents
36.
KOEBNER PHENOMENA
• localizednon specific trauma provokes lesions of a dermatosis which is spontaneously present
‐
elsewhere, and in ‘active’ or eruptive phase.
• Lesions are frequently linear (scratching)
• Psoriasis, lichen planus, lichen nitidus, vitiligo, lichen sclerosus, pityriasis rubra pilaris
Pseudo- Koebner phenomena
Inoculation of infective agent in an area of
traumatised skin
Warts molluscum contagiosum
Reverse Koebner phenomena
Clearing of established cutaneous lesion with
injury- psoriasis
WOOD’S LAMP
A Wood’slamp is a mercury vapor ultraviolet lamp with an incorporated
Wood’s filter (barium silicate glass with 9% nickel oxide) which is
opaque to all wavelengths except those between 320 and 400 nm. It
primarily emits the 360 nm wavelength.