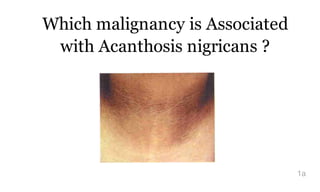
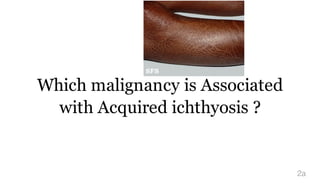
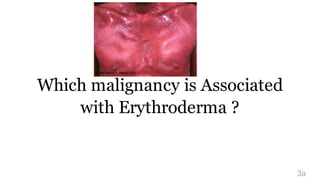
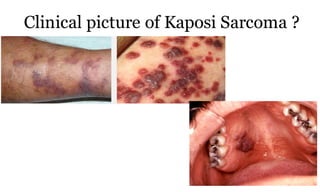

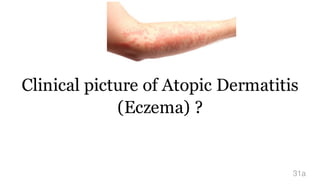
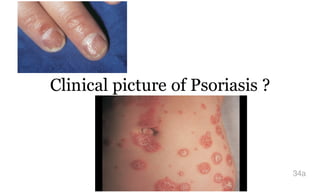

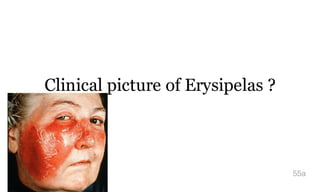
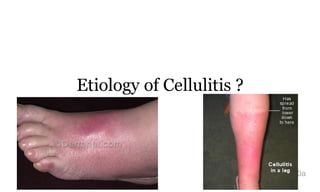
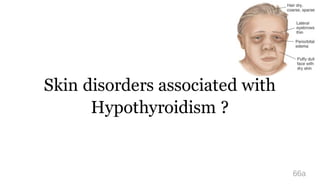
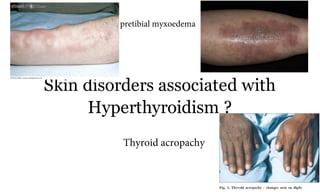

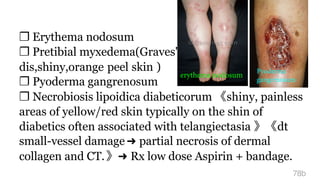
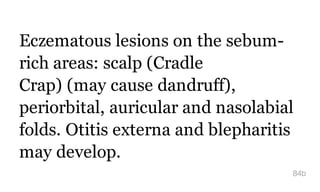


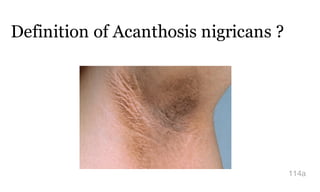







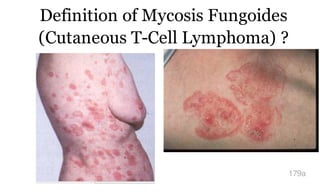
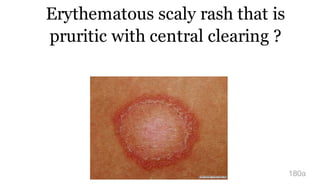
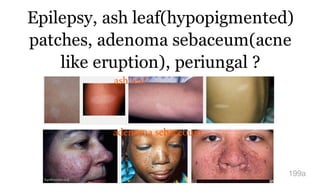
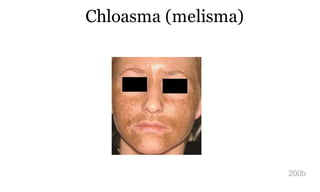

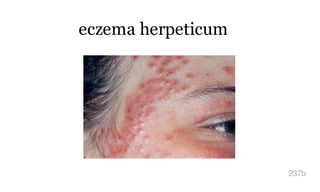



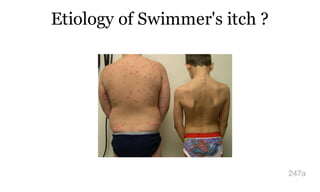



This document provides summaries of various dermatological conditions and malignancies. It discusses the associations, clinical pictures, diagnostic tests, and treatments for conditions like acanthosis nigricans, acquired ichthyosis, erythroderma, malignant melanoma, basal cell carcinoma, Kaposi sarcoma, atopic dermatitis, psoriasis, pemphigus vulgaris, bullous pemphigoid, porphyria cutanea tarda, impetigo, and erysipelas. For each condition, it concisely outlines the key identifying features, diagnostic approaches, and therapeutic options.























































































