Download to read offline


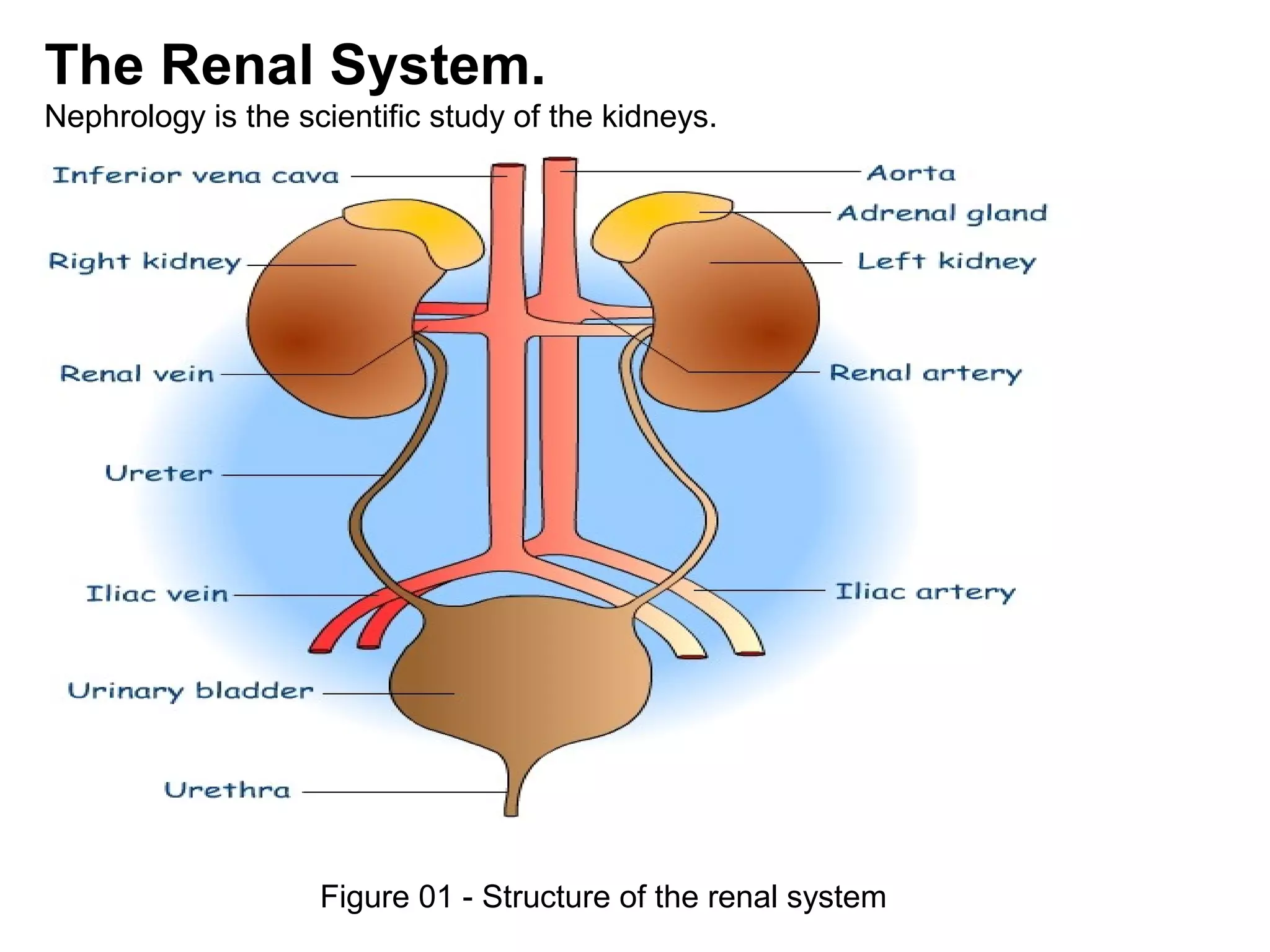


















The Department of Clinical Pharmacy at the University of Calabar Teaching Hospital aims to develop expertise in several areas of specialized pharmaceutical care such as pediatrics, cardiology, HIV/AIDS, and oncology. Its vision is to become a center of excellence in these areas within five years. The document outlines the steps involved in clinical assessment of patients, providing pharmaceutical care, and evaluating treatment, which includes collecting patient data, identifying health issues, creating a care plan, monitoring outcomes, and documenting services. It also discusses renal system anatomy and functions, diseases that may be studied, and general genitourinary examination findings.
































![REPORT OF OYO SEMO[1]](https://cdn.slidesharecdn.com/ss_thumbnails/a95e2894-e255-461a-8e98-3a720a71e542-160128213224-thumbnail.jpg?width=640&height=640&fit=bounds)




















































