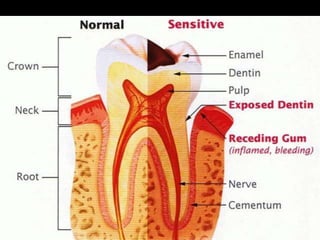
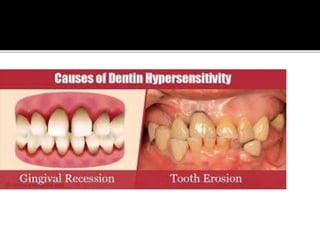
This document discusses dental hypersensitivity. It defines hypersensitivity as pain from exposed dentin in response to stimuli that cannot be explained by dental defects or pathology. Approximately one in seven people experience hypersensitivity. Common causes include loss of enamel from factors like toothbrushing abrasion or dietary erosion. Theories on the mechanisms of hypersensitivity include direct nerve stimulation in dentinal tubules or fluid movement within tubules stimulating nerve endings in the pulp. Treatment options include agents and procedures that occlude dentinal tubules like calcium hydroxide or iontophoresis to block nerve activity and reduce sensitivity.