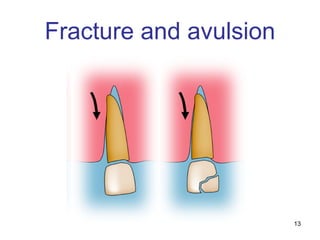
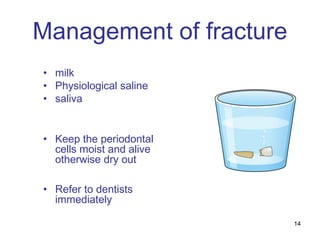
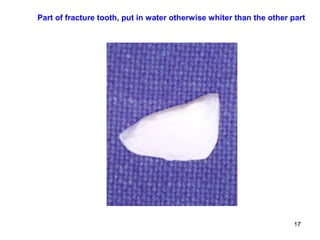
The document discusses various dental emergencies and their management, highlighting surveys conducted on the responses of Hong Kong primary and secondary school teachers and students about actions to take during dental injuries. It details causes and types of dental trauma, including fractures and avulsions, and emphasizes the importance of immediate care such as keeping periodontal cells moist and timely referrals to dentists. Additionally, it covers complications from dental infections, including cavernous sinus thrombosis and brain abscesses, with implications for treatment and prevention.



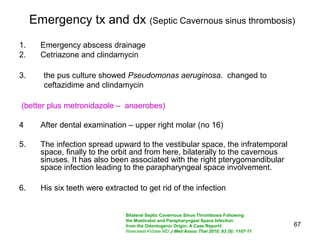
![12
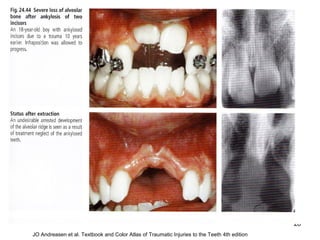
JO Andreasen et al. Textbook and Color Atlas of
]Traumatic Injuries to the Teeth 4th edition](https://image.slidesharecdn.com/linkedinppttotuenmunhospital15-180729040046/85/Dental-Emergencies-12-320.jpg)



































![References
128
JO Andreasen et al. Textbook and Color Atlas of
]Traumatic Injuries to the Teeth 4th edition
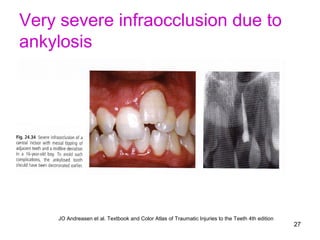
JO Andreasen et al. Textbook and Color Atlas of Traumatic Injuries to the Teeth 4th edition P473
JO Andreasen et al. Textbook and Color Atlas of Traumatic Injuries to the Teeth 4th edition
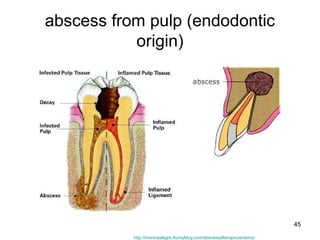
http://midcitysecuritydistrict.org/baptism-important-facts-about-hinduism-in-the-classical-period](https://image.slidesharecdn.com/linkedinppttotuenmunhospital15-180729040046/85/Dental-Emergencies-128-320.jpg)
















































































![Cells and Organs of immune system [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/cellsandorgansofimmunesystemautosaved-260123152717-ea0cb261-thumbnail.jpg?width=640&height=640&fit=bounds)





