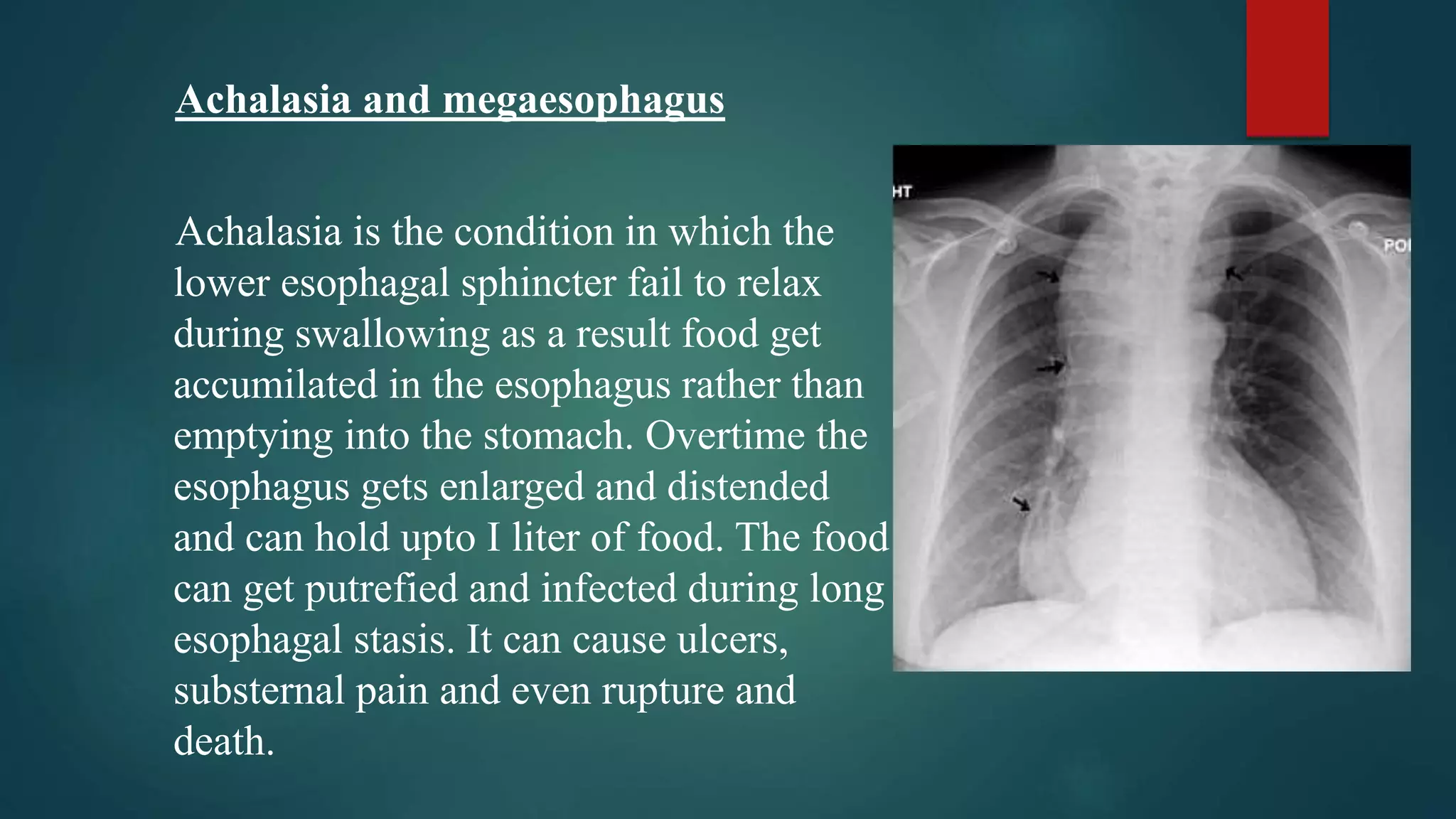
The document discusses the complex neurological and anatomical processes involved in normal deglutition, or swallowing, including the structures, sequence of events, and neural control of moving food from the mouth to the stomach. It also covers disorders that can occur if this coordinated process is disrupted, such as achalasia where the lower esophageal sphincter fails to relax properly.







































































![4 swallowing Dr. Ahed[1].pptx [Read-Only].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/4swallowingdr-250421223242-efb3095d-thumbnail.jpg?width=640&height=640&fit=bounds)











![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)















