Download as PDF, PPTX




![CRC: Epidemiology in 2013
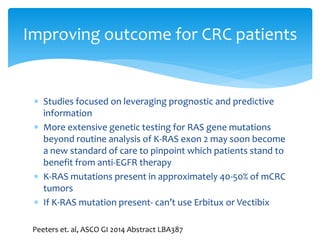
Fourth most common cancer
diagnosis in US[1]
Estimated 142,820 new cases in
2013; 1:1 male:female ratio[2]
Second leading cause of cancer
deaths in 2013 (estimated 50,830
deaths)[1]
Steady decrease in age-adjusted
incidence rates of distal colon,
proximal colon, and rectal cancers
in 1976-2005[4]
Death Rates in 2008,
per 100,000[3], %
Male
Female
All races
20.2
14.1
White
19.5
13.6
Black
29.8
19.8
Asian/Pacific Islander
13.1
9.6
American Indian/ Alaska
Native
18.8
14.6
Hispanic
15.3
10.2
1. American Cancer Society. Cancer facts & figures. 2013. 2. Siegel R, et al. CA Cancer
J Clin. 2012;62:10-29. 3. SEER. Stat fact sheets: colon and rectum. 4. Cheng L, et al. Am Clin Oncol.
2011;34:573-580.](https://image.slidesharecdn.com/ccawebinarpersonalizedcrccarefeb2014-140219150033-phpapp02/85/RESEARCH-TREATMENT-NEWS-Highlights-from-the-2014-GI-Cancer-Symposium-9-320.jpg)
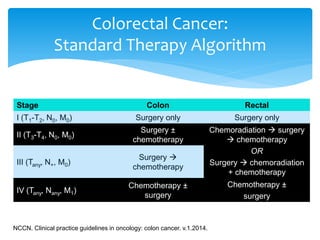

The document discusses the 2014 updates in personalized medicine for colorectal cancer, highlighting initiatives from the Colon Cancer Alliance and Fight Colorectal Cancer. It includes data on cancer incidence, demographics, and highlights advancements in treatment options, such as the Oncotype DX test's impact on treatment decisions and the effectiveness of various therapies. The document also emphasizes the importance of early detection, personalized treatment approaches, and ongoing support for patients and their families.
























































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)








