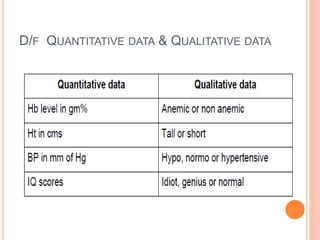
This document defines different types of data and how they are collected and presented. It discusses qualitative vs quantitative data, primary vs secondary data, and nominal vs ordinal data. It also describes key sources of health data like the census, sample registration system, hospital records, and surveys. Finally, it covers principles of data presentation through tables, bar diagrams, histograms and other charts. The key sources of health data in India include the census conducted every 10 years, sample registration system for vital events, and data from hospitals, disease notification systems and surveys.