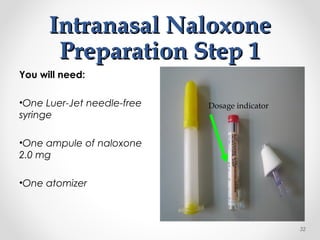
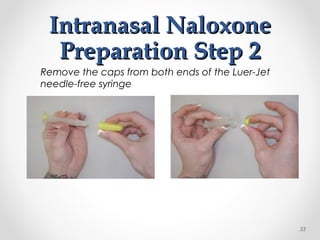
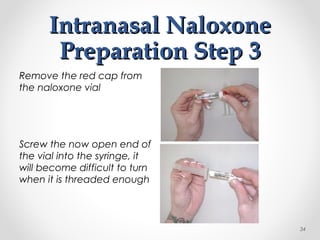
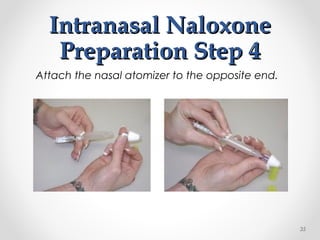
This document provides training for EMTs and EMRs on administering the opioid antagonist naloxone. It aims to reduce deaths from opioid overdose by instructing first responders. The training covers recognizing and treating opioid overdose, indications and contraindications for naloxone use, possible adverse reactions, and how to prepare and administer naloxone via intramuscular autoinjector or intranasal spray. Responders learn to identify overdose, administer naloxone, manage adverse reactions, and ensure transportation to definitive care.