COSHH RISK ASSESSMENT Form # HSEQ - COSHHRA Rev 3.doc

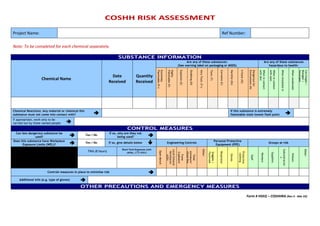
Project Name: Ref Number: Note: To be completed for each chemical separately. SUBSTANCE INFORMATION Chemical Name Date Received Quantity Received Are any of these substances: (See warning label on packaging or MSDS) Are any of these substances hazardous to health: Extremely Flammable (F+) Highly Flammable (F) Explosive (E) Oxidising (O) Very Toxic (T+) Toxic (T) Corrosive (C) Harmful (Xn) Irritant (Xi) Dangerous for Environment (N) When in contact with skin When in contact with eyes When breathed in When swallowed Carcinogen / Mutagen / Teratogen Chemical Reactions: Any material or chemical this substance must not come into contact with? If this substance is extremely flammable state lowest flash point If appropriate, work only to be carried out by these named people CONTROL MEASURES Can less dangerous substance be used? Yes / No If so, why are they not being used? Does this substance have Workplace Exposure Limits (WEL)? Yes / No If so, give details below Engineering Controls Personal Protective Equipment (PPE) Groups at risk TWA (8 hours) Short Term Exposure Limit (STEL) (15 min) Open Bench Local Exhaust Ventilation (LEV) Fume Cupboard Total enclosure/ Glove Box Other: Goggles / Facemask Respirator Gloves Protective clothing Staff Workers Suppliers Subcontractors Visitors Other: Controls measures in place to minimise risk Additional info (e.g. type of gloves) OTHER PRECAUTIONS AND EMERGENCY MEASURES First Aid: What Action should be taken if this substance is: How should an accidental release / spillage be dealt with? Swallowed: In contact with Skin: Fire Precautions: What actions will be taken in the event of a fire involving this substance? In contact with Eyes: Disposal: How should this substance be disposed of? Breathed in: Sources of Information (e.g. Suppliers MSDS) Is heath surveillance required? Yes / No Is training required for this process? Yes / No DECLARATION REASSESSMENT Assessment completed By: Name: Signature: Date: Date for reassessment Review Date Reviewed By Supervisor: Name: Signature: Date: HSE In Charge: Name: Signature: Date:

Recommended
Recommended
More Related Content
Similar to COSHH RISK ASSESSMENT Form # HSEQ - COSHHRA Rev 3.doc
Similar to COSHH RISK ASSESSMENT Form # HSEQ - COSHHRA Rev 3.doc (6)
More from Dwarika Bhushan Sharma
More from Dwarika Bhushan Sharma (20)
Recently uploaded
Recently uploaded (20)
COSHH RISK ASSESSMENT Form # HSEQ - COSHHRA Rev 3.doc
- 1. COSHH RISK ASSESSMENT Form # HSEQ – COSHHRA (Rev 3 - Mar 23) Project Name: Ref Number: Note: To be completed for each chemical separately. SUBSTANCE INFORMATION Chemical Name Date Received Quantity Received Are any of these substances: (See warning label on packaging or MSDS) Are any of these substances hazardous to health: Extremely Flammable (F+) Highly Flammable (F) Explosive (E) Oxidising (O) Very Toxic (T+) Toxic (T) Corrosive (C) Harmful (Xn) Irritant (Xi) Dangerous for Environment (N) When in contact with skin When in contact with eyes When breathed in When swallowed Carcinogen / Mutagen / Teratogen Chemical Reactions: Any material or chemical this substance must not come into contact with? If this substance is extremely flammable state lowest flash point If appropriate, work only to be carried out by these named people CONTROL MEASURES Can less dangerous substance be used? Yes / No If so, why are they not being used? Does this substance have Workplace Exposure Limits (WEL)? Yes / No If so, give details below Engineering Controls Personal Protective Equipment (PPE) Groups at risk TWA (8 hours) Short Term Exposure Limit (STEL) (15 min) Open Bench Local Exhaust Ventilation (LEV) Fume Cupboard Total enclosure/ Glove Box Other: Goggles / Facemask Respirator Gloves Protective clothing Staff Workers Suppliers Subcontractor s Visitors Other: Controls measures in place to minimise risk Additional info (e.g. type of gloves) OTHER PRECAUTIONS AND EMERGENCY MEASURES
- 2. COSHH RISK ASSESSMENT Form # HSEQ – COSHHRA (Rev 3 - Mar 23) First Aid: What Action should be taken if this substance is: How should an accidental release / spillage be dealt with? Swallowed: In contact with Skin: Fire Precautions: What actions will be taken in the event of a fire involving this substance? In contact with Eyes: Disposal: How should this substance be disposed of? Breathed in: Sources of Information (e.g. Suppliers MSDS) Is heath surveillance required? Yes / No Is training required for this process? Yes / No DECLARATION REASSESSMENT Assessment completed By: Name: Signature: Date: Date for reassessment Review Date Reviewed By Supervisor: Name: Signature: Date: HSE In Charge: Name: Signature: Date: