Downloaded 58 times

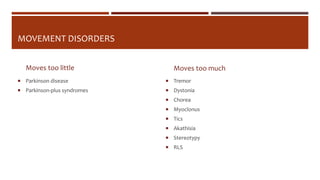
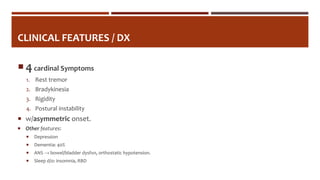


This document discusses Parkinson's disease, a common neurodegenerative movement disorder affecting approximately 1% of individuals over 60, with a focus on its clinical features, differential diagnoses, and treatment options. It outlines the pathophysiology, symptoms like tremor, rigidity, and bradykinesia, and various medications including l-dopa-carbidopa and dopamine agonists, as well as the implications of deep brain stimulation (DBS). Additionally, it provides clinical scenarios for diagnosis and treatment decision-making.





































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)

















