Download to read offline
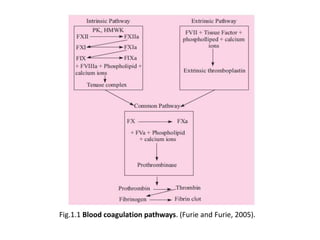
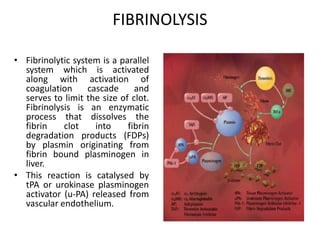
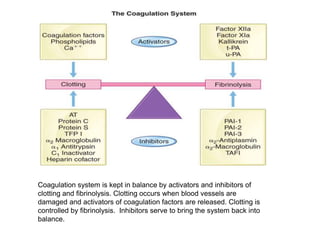
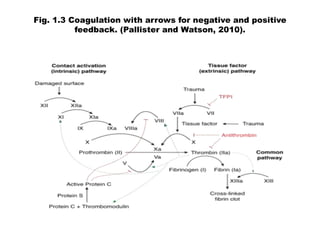

The document discusses the control of coagulation through various proteins and pathways that regulate clot formation and dissolution. Coagulation begins with tissue factor activating the coagulation cascade to form a clot. This is regulated by tissue factor pathway inhibitor and proteins that inhibit specific coagulation factors, such as protein C inhibiting factors V and VIII. Clot dissolution is mediated by plasmin and inhibited by alpha2-antiplasmin. Together these pathways maintain a balance between clot formation and removal. Deficiencies can lead to bleeding disorders or thrombosis.



































































