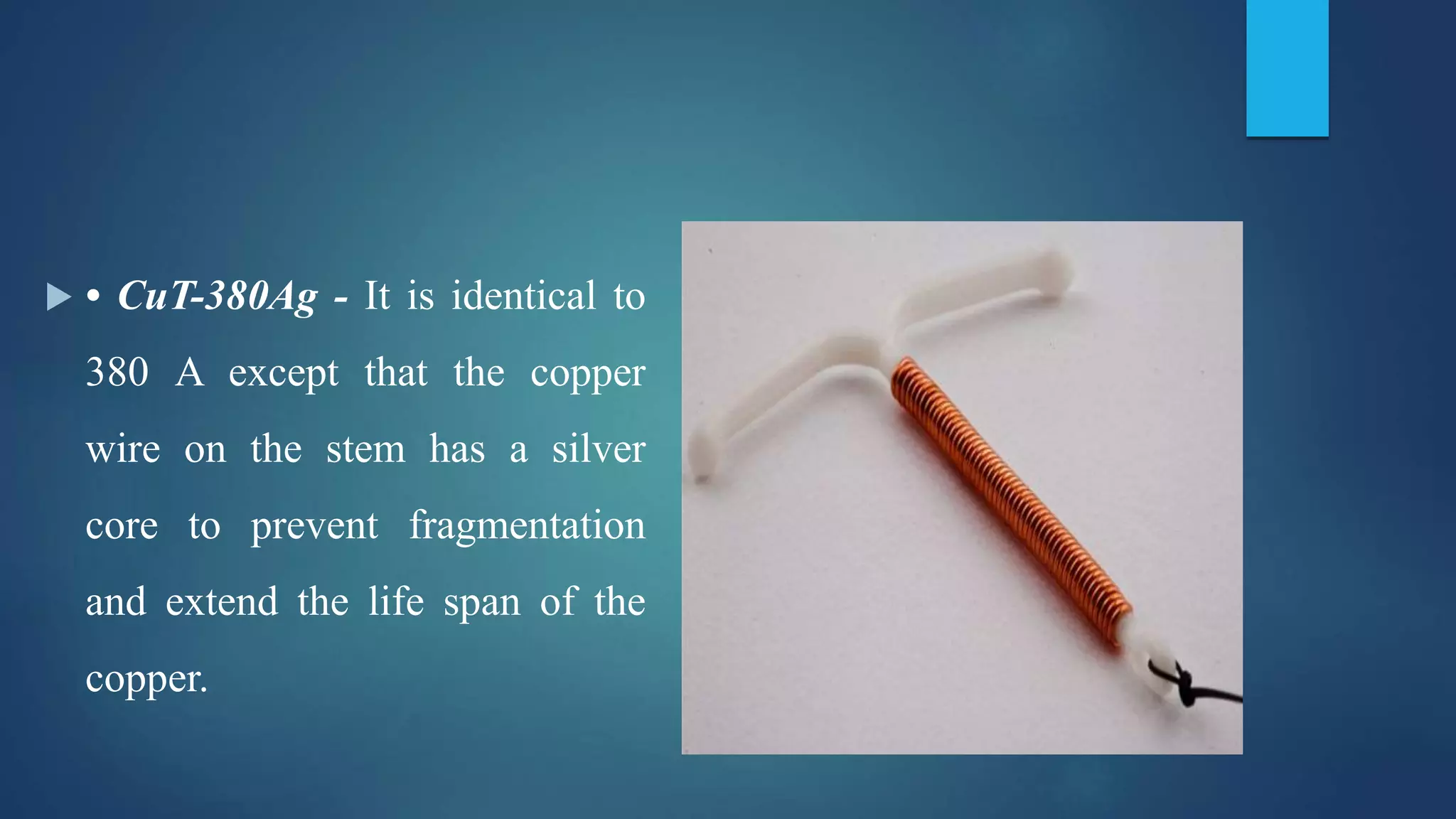
The document provides an overview of various contraceptive methods, categorizing them into spacing and terminal methods. It details barrier methods, hormonal contraceptives, intrauterine devices (IUDs), and emergency contraception, discussing their advantages, disadvantages, and effectiveness. Key methods include male and female condoms, diaphragms, hormonal pills, and IUDs, with emphasis on their use in preventing unwanted pregnancies and sexually transmitted diseases.