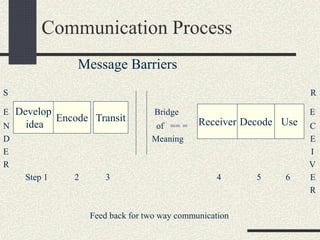
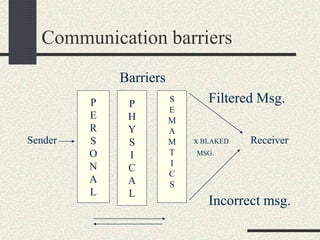
This document discusses communication skills in nursing. It defines communication and describes it as a process of exchanging information between individuals through symbols, signs or data. Good communication is important in nursing as it allows nurses to get their point across, inform patients, build rapport, educate, and promote understanding which helps in treatment. Communication can be verbal through speaking and listening, or non-verbal through body language, facial expressions, and other means. The document outlines various theories of communication and discusses interpersonal, intrapersonal, and group communication. It also describes the essential components of communication including the sender, message, channel, receiver and feedback. Barriers to effective communication and best practices for communication in nursing are also covered.