Candidacy for CI & off label.pptx for candidate selection
1.
History of CochlearImplants
1800 Alessandro Volta.
1957 Djourno and Eyries.
1961 Dr. Wiliam F House.
1970s.
1984 FDA approved single channel device in adults.
2.
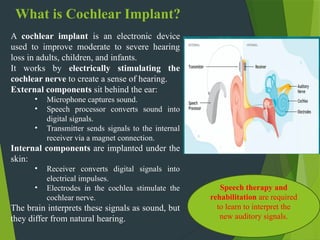
What is CochlearImplant?
A cochlear implant is an electronic device
used to improve moderate to severe hearing
loss in adults, children, and infants.
It works by electrically stimulating the
cochlear nerve to create a sense of hearing.
External components sit behind the ear:
• Microphone captures sound.
• Speech processor converts sound into
digital signals.
• Transmitter sends signals to the internal
receiver via a magnet connection.
Internal components are implanted under the
skin:
• Receiver converts digital signals into
electrical impulses.
• Electrodes in the cochlea stimulate the
cochlear nerve.
The brain interprets these signals as sound, but
they differ from natural hearing.
Speech therapy and
rehabilitation are required
to learn to interpret the
new auditory signals.
3.
Current Implant Technology
Thethree companies currently have FDA approved implants:
Advanced Bionics (California) - HR90 K
Cochlear (Australia) - Nucleus 5
Med-El (Austria) - Sonata ti100
4.
Candidacy for CI- Children
• Candidacy for CI has changed gradually but
significantly since the first multichannel devices
were implanted in the late 1970s .
• Due to increasing experience, improvement of
technology and the proven reliability, the selection
criteria has broadened with shifting borders.
• Main extensions are related to age, additional
handicaps, residual hearing & special etiologies of
deafness.
• The obvious goal for careful selection of CI patients
is to never have a single patient perform more poorly
with their CI than they did with their hearing aids
(Gifford,H 2011)
5.
FDA approval forimplanting children:
1990 > 2 years
1998 = 18 months
2000 = 12 months
Changes in age of implantation are due to:
1. Better/early identification of HL (universal hearing screening)
2. Increased professional awareness
3. Changes in technology: Electrode array, programming, processors, telemetry.
6.
Stages in PatientSelection
Questionnaire
Age
Etiology
Onset of HL ( pre, peri, postlingual )
Duration of sensory deprivation (plasticity), Hearing aid use
Audiological investigations
Speech & Language evaluation
Psychological assessment IQ testing
Medical & Otological examination
Radiological examination
Vestibular testing
Electrical stimulation of the cochlea
7.
Audiological Evaluation
Behavioralaudiometry (age appropriate)
Aided free field testing
Tympanometry & acoustic reflexes
OAE
ABR
Ear specific and frequency specific ASSR
Special tests : EABR, EAMLR, ESR,
Electrical late event related potentials
8.
Audiological Evaluation
(contd.)
Audiometricthresholds for children aged 12-23 months
hearing threshold for both ears should equal or exceed 90 dB.
For individuals older than 24 months hearing threshold should
equal or exceed 70 dB.
Speech detection with fit hearing aids in a sound field equal to
or worse than 55 dB.
Hearing aid trial for 3 months.
During HA trial, child should be making at least month to
month auditory progress as well as speech and language
progress. If this is not the case then, CI evaluation should be
considered (Gifford, H 2011)
9.
Audiological Evaluation
(contd.)
Theliterature has demonstrated that in terms of speech
development and language acquisition, the best results come
from children implanted under the age of 2 years similar to
normal hearing children (Sharma et. al. 2002)
All CI devices can be safely indicated for children 12 months or
older
However implanting children younger than 12 months remains
controversial.
Further reductions in age at implantation are currently limited
by the nature of audiologic testing in very young children.
In cases of HL due to meningitis or hereditary hearing loss,
implantation should be considered before the age of 12 months.
10.
Other Evaluations and
Procedures
•Speech and Language Assessment.
Psychological Assessment, IQ Testing.
Counseling, family support, motivation and
realistic expectations.
Medical and Otological examination.
Radiological assessment:
CT
MRI
11.
Vaccination
Children withcochlear implants are at higher risk for meningitis, though
overall rate is low (<0.6%)
Streptococcus pneumoniae has been the most common organism
isolated in the children with cochlear implants who developed
meningitis
Current vaccine recommendation:
Patients <2 years old
• Prevnar(7-valent)only
Patients 2-5 years old
• Prevnar and Pneumovax (23-valent)
Patients >5 years old
• Pneumovax only
Additionally ,all patients <5years old should receive the Hib vaccine
Vaccination should be completed at least 2 weeks prior to surgery
12.
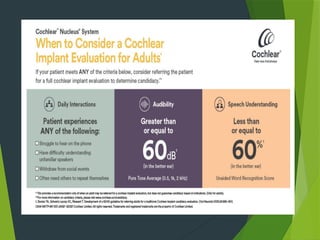
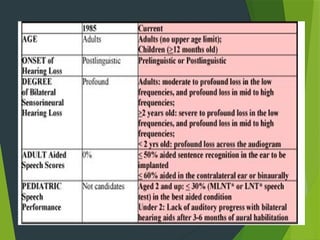
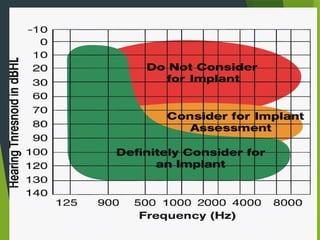
Candidacy for CI- Adults
Bilateral severe to profound sensorineural
hearing loss.
Limited benefit from appropriate hearing aids
i.e. poor speech recognition.
Speech recognition testing is the cornerstone
in adult CI patient selection, where the best-
aided scores on open-set sentence tests of
<50% in the ear to be implanted and <60% in
contralateral ear is considered as an indication
for implantation.
Telephone use is difficult, limited or impossible.
Patients is distressed by the inability to
communicate efferently on a daily basis.
No medical contraindications.
15.
According toGifford & Dorman, 2008 adult patients can have only
moderate hearing loss in the low frequencies, sloping to profound loss
in the mid to high frequencies, and still be excellent candidates for a
cochlear implant.
It is no longer a requirement that one have "no useable hearing." Aided
sentence recognition of 50% or less in the ear to be implanted and 60%
or less in the contralateral ear or bilaterally ("best aided condition") is
the current criterion for adults.
Age criteria for candidacy- The advantage of implanting an infant who
is still in the critical language acquisition stage may seem obvious, but
what about the 82-year-old who is socially isolated by a hearing loss?
Older adults show no increase in operative time or length of stay in the
hospital (Labadie, Carrasco, Gilmer, & Pillsbury, 2000).
Speech perception in the implanted elderly is comparable to that of
younger recipients (Kelsall, Shallop, & Burnelli, 1995;Vermeire, et al.,
2005). Cochlear implants have a significant positive impact on the
quality of life of older patients (Francis, Chee, Yeagle, Cheng and
Niparko, 2002). There is no upper age limit for cochlear implant
candidacy.
18.
Choosing the Most
AppropriateEar
Audiological Factors :
Residual hearing In the early years of CI , the audiologically
worse ear was chosen so that (un) expected iatrogenic
cochlear damage would have fewer consequences.
In the late 1990s the better ear with most residual hearing was
preferred as studies had shown that better result after CI.
Duration of HL It is generally accepted that duration of
deafness has a negative effect on CI performances. Most
clinicians choose the ear with the shortest duration of
deafness.
Only functioning labyrinth.
19.
Surgical Factors:
AnatomicVariations : Cochlear ossification, cochlear malformation and cochlear
nerve malformation.
Otological Medical History: Otitis media, cholesteatoma and temporal bone
fracture.
Personal Factors:
Handedness (right ear advantage)
20.
Contraindications for
Implantation
Completelyatretic VIII nerve
Small internal auditory canal syndrome
Agenesis of cochlea: Michel deformity
Active middle ear/mastoid infection
Tympanic membrane perforation
Severe organic brain dysfunction
Severe intellectual disability
Psychosis, unrealistic expectations
21.
Hybrid CI (ElectroAcoustic
Stimulation)
A hybrid cochlear implant (Hybrid CI) combines acoustic
hearing (like a hearing aid) with electrical stimulation (like a
traditional cochlear implant).
The expanded criteria have led to research questions centering
on advanced uses of the technology.
Specifically, could an implant benefit other users previously
not considered.
A group that was felt to be underserved with convention
amplification were those patients with the following
audiometric profile.
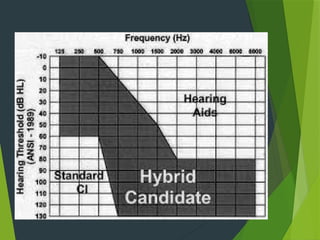
23.
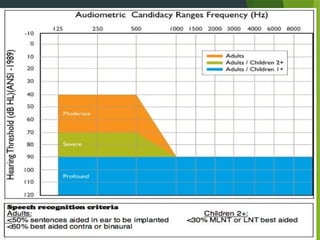
Audiogram:
Below 1.5kHz – No or moderate HL
Above 1.5 kHz – Severe to profound sensorineural hearing impairment.
Dead regions of the cochlea (elderly).
Speech Scores:
The patient's monosyllable word score should be <60% at 65 db SPL in the best
aided condition.
24.
Hearing Preservation Surgery
Twomethods are commonly used for inserting the electrode into
the cochlea:
Round-window insertion vs Cochleostomy insertion.
Round-window insertion has found a wider acceptance
because it is considered to be less traumatic (controversial)
25.
AS Electrodes forCochlear
Implants
• Long-term research has shown that mechanical flexibility of
the electrode array is one of the key factors for preserving
residual hearing.
Studies with different lengths of electrodes have shown that an
insertion depth of 10 mm has good chance of preserving
residual.
Electrodes that can be inserted to a depth of 18-20 mm are a
good compromise.
26.
EAS Audio Processors
Combines cochlear implant technology with a digital hearing
aid. This device uses one microphone for the input, but has two
separate digital sound processors for differentiated processing.
The parallel processing of these signals, however is performed
separately and optimized for both acoustic hearing (focusing
on low-frequency hearing) and cochlear implant stimulation
(focusing on high-frequency hearing).
The hearing aid is integrated in the ear hook and the amplified
signals are forwarded to the auditory pathway via an ear
mould.
The ear mould used for the acoustic component is similar to a
conventional hearing aid ear mould can be exchanged.
27.
Bilateral CI
RecentTrend towards BILATERAL use of CI/s
1992: 0-1%
2007: 14-15%
70% of bilateral CI usage is among 18 years and under age group.
Simultaneous CI
Sequential CI
28.
Advantages of bilateral
implantation
Improved hearing in quiet (binaural summation)
Improved hearing in noise (binaural squelch, head
shadow effect, and binaural redundancy)
Improved sound lateralization
Assurance that the better hearing is “captured’’
Qualitative listening improvement (more “balanced,
richer quality, more confident’’ feeling and less fatigued)
29.
Why Expand Candidacy?
Advances in electrode and processor technology.
Improved surgical techniques and rehabilitation outcomes.
Benefit shown in milder, asymmetric, and SSD cases.
Earlier implantation improves speech, language and QOL outcomes.
60/60 Guideline
Zwolan et al recommends that patients be considered for a cochlear implant
candidacy evaluation (CICE) if they obtain a score less than or equal to 60% correct
on an unaided monosyllabic word test in the better ear and if they demonstrate a PTA
greater than or equal to 60 dB HL.
The group is hopeful that this simple guideline will result in an increase in the
number of patients who are referred for a traditional cochlear implant candidacy
evaluation.
30.
Recent internationalsystematic review and consensus process,
establishing a standard of care for the treatment of adult patients
with unilateral cochlear implant for bilateral severe, profound, or
moderate sloping to profound sensorineural hearing loss.
It also includes a review of “Terry Zwolan et al Development of
a 60/60 Guideline for Referring Adults for a Traditional Cochlear
Implant Candidacy Evaluation. Otology & Neurotology: April
20, 2020.”
31.
Current Expanded Indications
Residual hearing: Hybrid/EAS implants preserve
low frequency hearing.
‑
Asymmetric hearing loss: CI in poorer ear + hearing aid
in better ear.
Single sided deafness (SSD): CI improves localization
‑
and tinnitus.
Pediatric implantation: now <9 months in select centers.
Older adults (>85 years): safe, effective, QOL
improvement.
33.
Off Label Candidacy
‑
Definition: Use beyond approved regulatory criteria but
supported by clinical data.
Examples:
Good contralateral ear (>60% WRS)
Moderate hearing loss with poor clarity
Post lingual SSD
‑
Cleveland Clinic 2024: 55% off label recipients had
‑
≥20% gain in speech scores.
34.
Surgical and Technological
Advances
Flexible, short electrode arrays enable hearing preservation.
Round window,
‑ soft surgery approaches reduce trauma.
‑
Electric acoustic stimulation (EAS): combines acoustic +
‑
electric hearing.
Smart processors with noise reduction and wireless
connectivity.
35.
Pediatric Advances
Earlyimplantation (<1 year) yields superior auditory and
language outcomes.
Bilateral implantation enhances localization and binaural
hearing.
Neural plasticity studies support early intervention.
Reference: Dettman SJ et al., Otol Neurotol 2023.
36.
Outcomes of
Expanded/Off LabelUse
‑
SSD/AHL: Improved sound localization, reduced tinnitus.
EAS: +20-30% better speech in noise performance.
‑ ‑
Older Adults: Improved QOL and cognition.
Pediatric: Higher CAP/SIR scores post CI.
‑
Evidence supports safe and effective off label outcomes.
‑
37.
Challenges and Considerations
Residual hearing loss risk despite
atraumatic surgery.
Off label:
‑ Reimbursement and approval
barriers.
Patient Counselling: Expectation
management vital.
Increased CI demand requires
audiology/rehab infrastructure.
38.
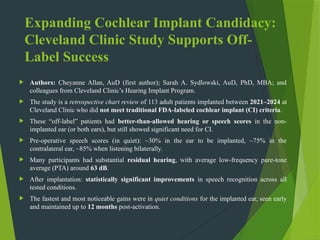
Expanding Cochlear ImplantCandidacy:
Cleveland Clinic Study Supports Off-
Label Success
Authors: Cheyanne Allan, AuD (first author); Sarah A. Sydlowski, AuD, PhD, MBA; and
colleagues from Cleveland Clinic’s Hearing Implant Program.
The study is a retrospective chart review of 113 adult patients implanted between 2021–2024 at
Cleveland Clinic who did not meet traditional FDA-labeled cochlear implant (CI) criteria.
These “off-label” patients had better-than-allowed hearing or speech scores in the non-
implanted ear (or both ears), but still showed significant need for CI.
Pre-operative speech scores (in quiet): ~30% in the ear to be implanted, ~75% in the
contralateral ear, ~85% when listening bilaterally.
Many participants had substantial residual hearing, with average low-frequency pure-tone
average (PTA) around 63 dB.
After implantation: statistically significant improvements in speech recognition across all
tested conditions.
The fastest and most noticeable gains were in quiet conditions for the implanted ear, seen early
and maintained up to 12 months post-activation.
39.
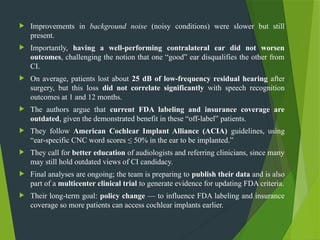
Improvements inbackground noise (noisy conditions) were slower but still
present.
Importantly, having a well-performing contralateral ear did not worsen
outcomes, challenging the notion that one “good” ear disqualifies the other from
CI.
On average, patients lost about 25 dB of low-frequency residual hearing after
surgery, but this loss did not correlate significantly with speech recognition
outcomes at 1 and 12 months.
The authors argue that current FDA labeling and insurance coverage are
outdated, given the demonstrated benefit in these “off-label” patients.
They follow American Cochlear Implant Alliance (ACIA) guidelines, using
“ear-specific CNC word scores ≤ 50% in the ear to be implanted.”
They call for better education of audiologists and referring clinicians, since many
may still hold outdated views of CI candidacy.
Final analyses are ongoing; the team is preparing to publish their data and is also
part of a multicenter clinical trial to generate evidence for updating FDA criteria.
Their long-term goal: policy change — to influence FDA labeling and insurance
coverage so more patients can access cochlear implants earlier.
40.
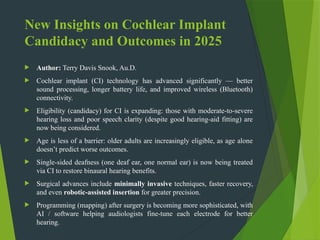
New Insights onCochlear Implant
Candidacy and Outcomes in 2025
Author: Terry Davis Snook, Au.D.
Cochlear implant (CI) technology has advanced significantly — better
sound processing, longer battery life, and improved wireless (Bluetooth)
connectivity.
Eligibility (candidacy) for CI is expanding: those with moderate-to-severe
hearing loss and poor speech clarity (despite good hearing-aid fitting) are
now being considered.
Age is less of a barrier: older adults are increasingly eligible, as age alone
doesn’t predict worse outcomes.
Single-sided deafness (one deaf ear, one normal ear) is now being treated
via CI to restore binaural hearing benefits.
Surgical advances include minimally invasive techniques, faster recovery,
and even robotic-assisted insertion for greater precision.
Programming (mapping) after surgery is becoming more sophisticated, with
AI / software helping audiologists fine-tune each electrode for better
hearing.
41.
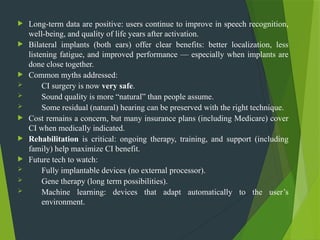
Long-term dataare positive: users continue to improve in speech recognition,
well-being, and quality of life years after activation.
Bilateral implants (both ears) offer clear benefits: better localization, less
listening fatigue, and improved performance — especially when implants are
done close together.
Common myths addressed:
CI surgery is now very safe.
Sound quality is more “natural” than people assume.
Some residual (natural) hearing can be preserved with the right technique.
Cost remains a concern, but many insurance plans (including Medicare) cover
CI when medically indicated.
Rehabilitation is critical: ongoing therapy, training, and support (including
family) help maximize CI benefit.
Future tech to watch:
Fully implantable devices (no external processor).
Gene therapy (long term possibilities).
Machine learning: devices that adapt automatically to the user’s
environment.
42.
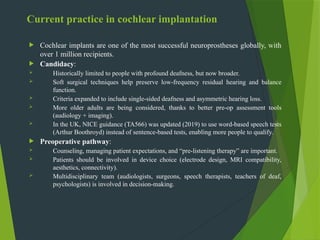
Current practice incochlear implantation
Cochlear implants are one of the most successful neuroprostheses globally, with
over 1 million recipients.
Candidacy:
Historically limited to people with profound deafness, but now broader.
Soft surgical techniques help preserve low-frequency residual hearing and balance
function.
Criteria expanded to include single-sided deafness and asymmetric hearing loss.
More older adults are being considered, thanks to better pre-op assessment tools
(audiology + imaging).
In the UK, NICE guidance (TA566) was updated (2019) to use word-based speech tests
(Arthur Boothroyd) instead of sentence-based tests, enabling more people to qualify.
Preoperative pathway:
Counseling, managing patient expectations, and “pre-listening therapy” are important.
Patients should be involved in device choice (electrode design, MRI compatibility,
aesthetics, connectivity).
Multidisciplinary team (audiologists, surgeons, speech therapists, teachers of deaf,
psychologists) is involved in decision-making.
43.
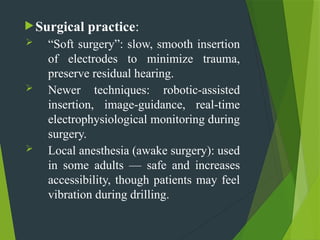
Surgical practice:
“Softsurgery”: slow, smooth insertion
of electrodes to minimize trauma,
preserve residual hearing.
Newer techniques: robotic-assisted
insertion, image-guidance, real-time
electrophysiological monitoring during
surgery.
Local anesthesia (awake surgery): used
in some adults — safe and increases
accessibility, though patients may feel
vibration during drilling.
44.
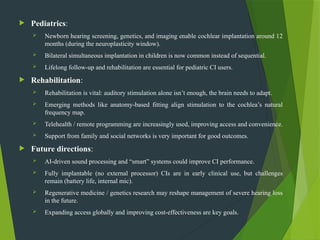
Pediatrics:
Newbornhearing screening, genetics, and imaging enable cochlear implantation around 12
months (during the neuroplasticity window).
Bilateral simultaneous implantation in children is now common instead of sequential.
Lifelong follow-up and rehabilitation are essential for pediatric CI users.
Rehabilitation:
Rehabilitation is vital: auditory stimulation alone isn’t enough, the brain needs to adapt.
Emerging methods like anatomy-based fitting align stimulation to the cochlea’s natural
frequency map.
Telehealth / remote programming are increasingly used, improving access and convenience.
Support from family and social networks is very important for good outcomes.
Future directions:
AI-driven sound processing and “smart” systems could improve CI performance.
Fully implantable (no external processor) CIs are in early clinical use, but challenges
remain (battery life, internal mic).
Regenerative medicine / genetics research may reshape management of severe hearing loss
in the future.
Expanding access globally and improving cost-effectiveness are key goals.
45.
Key Takeaways
Candidacyevolving from 'Audiogram based' to 'Functional
‑
Limitation' model.
Off label use is evidence driven and beneficial in select cases.
‑ ‑
Early identification and multidisciplinary care are essential.
ENT-Audiology collaboration maximizes outcomes.
#6 The literature has demonstrated that in terms of speech development and language acquisition , the best results come from children implanted under the age of 2 years similar to normal hearing children (Sharma et all 2002
#13 History :
Onset & course of hearing loss
Duration (plasticity)
Aetiology ( fever , trauma )
History of HA use
Means of communication
Education
Motivation , realistic expectations Prelingual adults
#16 HINT TEST IS PRESENTED IN QUITE ROOM AND RECORDED RESPONSE
#33 The FDA’s move in 2020 to lower the approved CI implantation age from 12 to 9 months








![Recent_Advances_Cochlear_Implant_Candidacy_Dr_Anand_Gupta[1]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/recentadvancescochlearimplantcandidacydranandgupta1-1-251128040227-e519dadb-thumbnail.jpg?width=640&height=640&fit=bounds)





![cochlear implant [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/cochlearimplantautosaved-230807191245-e9fc2957-thumbnail.jpg?width=640&height=640&fit=bounds)



















![Introduction to hearing implairment & cochlear implantation]](https://cdn.slidesharecdn.com/ss_thumbnails/introductiontohearingimplairmentcochlearimplantation-161111054000-thumbnail.jpg?width=640&height=640&fit=bounds)
![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)


















