
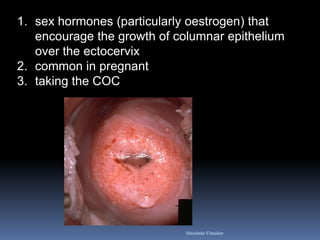
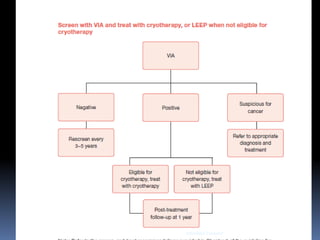
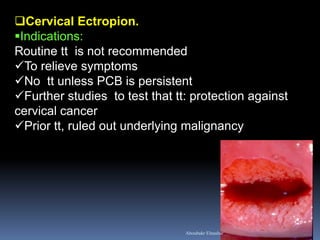
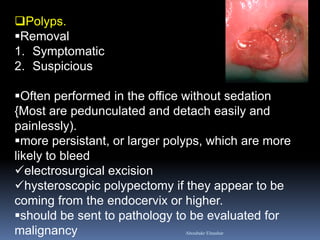
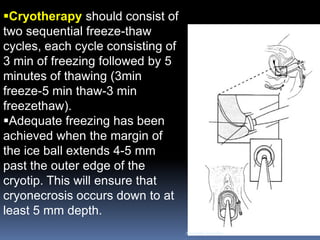
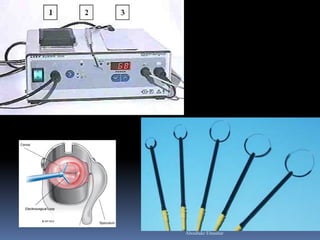
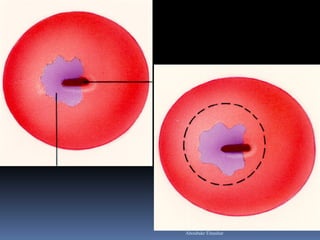
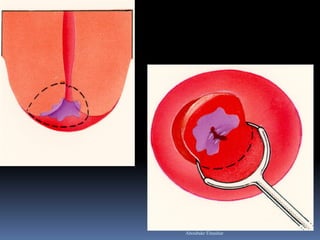
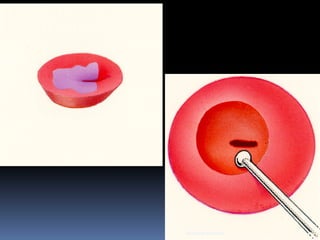

The document discusses abnormal-looking cervix (suspicious cervix). It defines the condition and lists potential causes such as infections, hormonal/nutritional factors, and neoplasms. Evaluation involves history, exam, tests for infections, cytology, colposcopy. Treatment depends on underlying cause but may include procedures like cryotherapy for pre-cancerous lesions. Screening programs in developing countries commonly use visual inspection with acetic acid followed by cryotherapy for pre-cancerous lesions detected.











































































































