Download to read offline












![CHAPTER 64 DRUGS USED IN ONCOLOGIC DISORDERS 929
effects, they should not be denied the potential benefits of • Mercaptopurine should be given in smaller doses
chemotherapy on the basis of age alone. Instead, greater vig- because the drug may be eliminated more slowly.
ilance is needed to maximize benefits and minimize hazards • Methotrexate is excreted mainly by the kidneys and its
of chemotherapy. For example, older adults are more sensi- use in clients with impaired renal function may lead to
tive to the neurotoxic effects of vincristine and need reduced accumulation of toxic amounts or additional renal dam-
dosages of some drugs (eg, cyclophosphamide, MTX) if age. The client’s renal status should be evaluated before
renal function is impaired. Creatinine clearance should be and during MTX therapy. If significant renal impair-
monitored; serum creatinine level is not a reliable indicator ment occurs, the drug should be discontinued or re-
of renal function in older adults because of their decreased duced in dosage until renal function improves.
muscle mass. In clients who receive high doses for treatment of os-
teosarcoma, MTX may cause renal damage leading to
acute renal failure. Nephrotoxicity is attributed to precip-
Use in Renal Impairment itation of MTX and a metabolite in renal tubules. Renal
impairment may be reduced by monitoring renal function
Some antineoplastic drugs are nephrotoxic (eg, cisplatin, MTX) closely, ensuring adequate hydration, alkalinizing the
and many are excreted through the kidneys. In the presence urine, and measuring serum drug levels.
of impaired renal function, risks of further impairment or ac- • Procarbazine may cause more severe adverse effects if
cumulation of toxic drug levels are increased. Thus, renal given to clients with impaired renal function. Hospital-
function should be monitored carefully during therapy and ization is recommended for the first course of treatment.
drug dosages are often reduced according to creatinine clear- Many other drugs should be used with caution in clients
ance (CrCl) levels. In advanced cancer, CrCl may not be with renal impairment. Asparaginase often causes azotemia
reliable because these clients are often in catabolic states char- (eg, increased BUN); acute renal failure and fatal renal in-
acterized by increased production of creatinine from break- sufficiency have been reported. Bleomycin is rarely associated
down of skeletal muscle and other proteins. Renal effects of with nephrotoxicity but its elimination half-life is prolonged in
selected drugs are as follows: clients with a CrCl of less than 35 mL/minute. Cytarabine is
• Carmustine and lomustine are associated with azotemia detoxified mainly by the liver. However, clients with renal im-
and renal failure, usually with long-term IV administra- pairment may have more CNS-related adverse effects, and
tion and large cumulative doses. dosage reduction may be needed. Gemcitabine should be used
• Cisplatin is nephrotoxic, and acute overdosage can with caution, although it has not been studied in clients with
cause renal failure. Because nephrotoxicity is increased preexisting renal impairment. Mild proteinuria and hematuria
with repeated doses, cisplatin is given at 3- or 4-week were commonly reported during clinical trials, and hemolytic-
intervals and renal function tests (eg, serum creatinine, uremic syndrome (HUS) was reported in a few clients. HUS
blood urea nitrogen [BUN]) and serum electrolytes may be manifested by anemia, indications of blood cell break-
(eg, sodium, potassium, calcium) are measured before down (eg, elevated bilirubin and reticulocyte counts), and renal
each course of therapy. Renal function is usually al- failure. The drug should be stopped immediately if HUS
lowed to return to normal before another dose is given. occurs; hemodialysis may be required.
Nephrotoxicity may be reduced by the use of amifostine
or IV hydration and mannitol.
• Cyclophosphamide may cause hemorrhagic ureteritis Use in Hepatic Impairment
and renal tubular necrosis with IV doses above 50 mg/kg.
These effects usually subside when the drug is stopped. Some antineoplastic drugs are hepatotoxic and many are me-
• Ifosfamide may increase BUN and serum creatinine, tabolized in the liver. In the presence of impaired hepatic
but its major effect on the urinary tract is hemorrhagic function, risks of further impairment or accumulation of toxic
cystitis, manifested by hematuria. Cystitis can be re- drug levels are increased. Dosage reduction is needed with
duced by the use of mesna, vigorous hydration, and de- some drugs and hepatic function should be monitored with
laying drug administration if a predose urinalysis shows most. However, abnormal values for the usual liver function
hematuria. tests (eg, serum aminotransferases such as aspartate amino-
• Irinotecan dosage should be reduced (eg, 0.75 mg/m2) transferase [AST] and alanine aminotransferase [ALT], biliru-
in clients with moderate impairment (CrCl 20 to bin, alkaline phosphatase) may indicate liver injury but do not
39 mL/minute). No dosage reduction is recommended indicate decreased ability to metabolize drugs. Clients with
with mild impairment (CrCl 40 to 60 mL/minute), and metastatic cancer often have impaired liver function.
there are inadequate data for recommendations in Hepatotoxic drugs include the anthracyclines (eg, doxoru-
severe impairment. bicin), mercaptopurine, MTX, paclitaxel, and vincristine. He-
• Melphalan should be reduced in dosage when given patic effects of these and selected other drugs are as follows:
IV, to reduce accumulation and increased bone marrow • Asparaginase is hepatotoxic in most clients and may
toxicity. It is unknown whether dosage reduction is increase preexisting hepatic impairment. It may also in-
needed with oral drug. crease hepatotoxicity of other medications. Signs of](https://image.slidesharecdn.com/clinicaldrugtherapynursingcapituloonco-101007145706-phpapp02/75/Clinical-drug-therapy-nursing-capitulo-onco-17-2048.jpg)

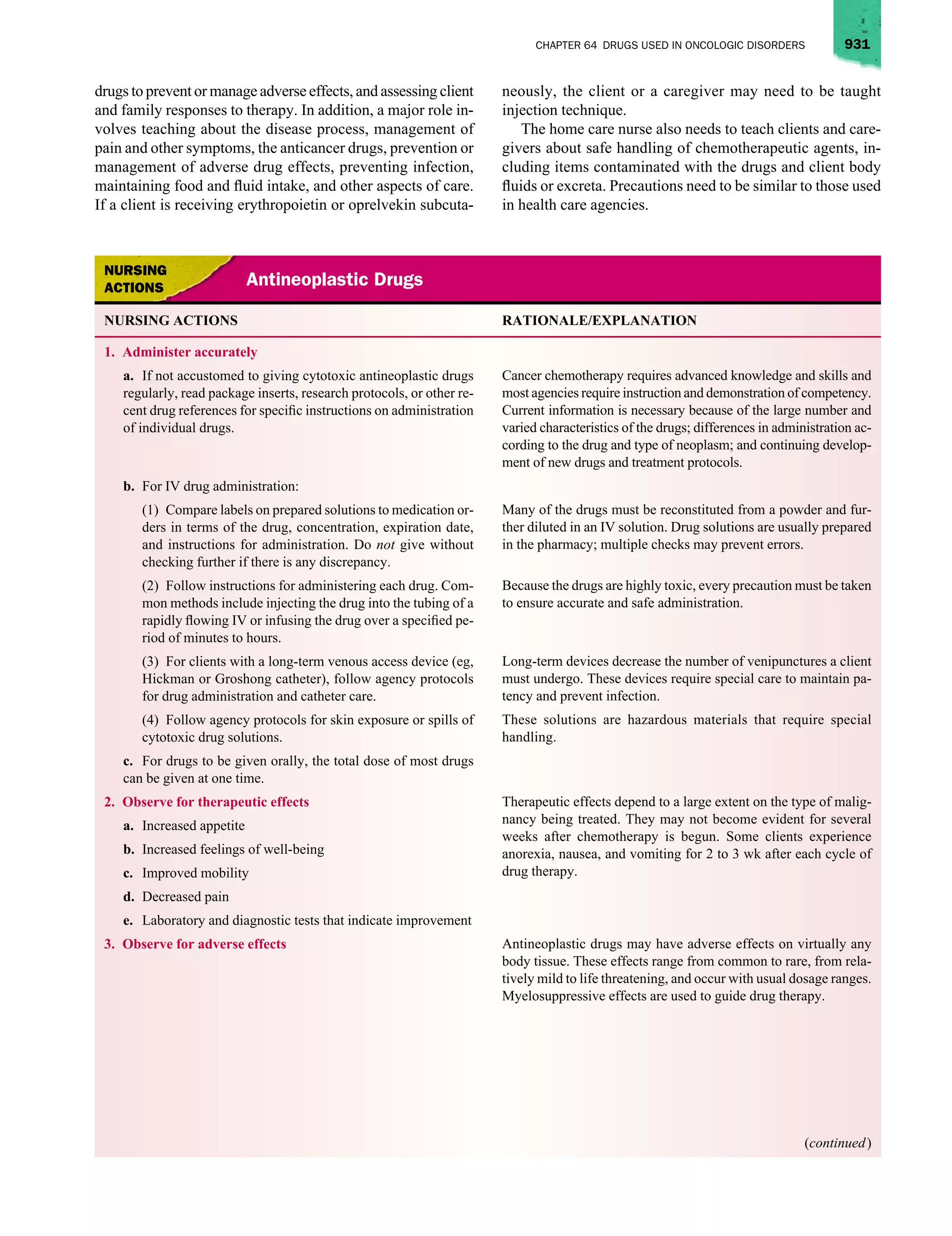
![932 SECTION 11 DRUGS USED IN SPECIAL CONDITIONS
NURSING ACTIONS RATIONALE/EXPLANATION
a. Hematologic effects:
(1) Bone marrow depression with leukopenia For most drugs, WBC and platelet counts reach their lowest points
(decreased white blood cell [WBC] count), thrombo- (nadirs) 7 to 14 d after drug administration and return toward nor-
cytopenia (decreased platelets), and anemia mal after 21 d. Normal leukocyte and platelet counts indicate re-
covery of bone marrow function. Anemia may occur later because
(decreased red blood cell [RBC] count, hemoglobin, the red blood cell lives longer than white cells and platelets.
and hematocrit)
(2) Decreased antibodies and lymphocytes Most of these drugs have immunosuppressant effects, which
impair body defenses against infection.
b. Gastrointestinal (GI) effects—anorexia, nausea, vomiting, Nausea and vomiting are very common, usually occur within a few
diarrhea, constipation, oral and intestinal mucositis and mu- hours of drug administration, and often subside within 12 to 24 h.
cosal ulcerations, oral candidiasis Constipation is most likely to occur with vincristine. Mucositis may
occur anywhere in the GI tract; may interfere with nutrition and
cause significant discomfort; may lead to infection, hemorrhage, or
perforation; and may require that drug therapy be stopped.
c. Integumentary effects—alopecia, dermatitis, tissue irrita- Complete hair loss may take several weeks to occur. Alopecia may
tion at injection sites cause psychological discomfort. Several drugs may cause phlebitis
and sclerosis of veins used for injections, as well as pain and tis-
sue necrosis if allowed to leak into tissues around the injection site.
d. Renal effects:
(1) Hyperuricemia and uric acid nephropathy When malignant cells are destroyed, they release uric acid into the
bloodstream. Uric acid crystals may precipitate in the kidneys and
cause impaired function or failure. Adverse effects on the kidneys
are especially associated with methotrexate and cisplatin. Hyper-
uricemia can be decreased by an ample fluid intake or by adminis-
tration of allopurinol.
(2) With cisplatin, nephrotoxicity (increased blood urea ni- Nephrotoxicity is a major adverse effect. Decreasing the dose or
trogen [BUN] and serum creatinine; decreased creatinine frequency of administration, vigorous hydration, and amifostine
clearance). administration can reduce the incidence.
(3) With cyclophosphamide or ifosfamide, hemorrhagic Hemorrhagic cystitis occurs in about 10% of clients. It is attributed
cystitis (blood in urine, dysuria, burning on urination) to irritating effects of drug metabolites on the bladder mucosa. The
drug is stopped if this occurs. Cystitis can be decreased by an ample
fluid intake. In addition, mesna is given with ifosfamide.
e. Pulmonary effects—cough, dyspnea, chest x-ray changes Adverse effects on the lungs are associated mainly with bleomycin
and methotrexate. With bleomycin, pulmonary toxicity may be
severe and progress to pulmonary fibrosis.
f. Cardiovascular effects—congestive heart failure (dyspnea, Cardiomyopathy is associated primarily with doxorubicin and re-
edema, fatigue), dysrhythmias, electrocardiographic changes lated drugs. This is a life-threatening adverse reaction. The heart
failure may be unresponsive to digoxin.
g. Central nervous system effects—peripheral neuropathy with This common effect of vincristine may worsen for several weeks
vincristine, manifested by muscle weakness, numbness and tin- after drug administration. There is usually some recovery of func-
gling of extremities, foot drop, and decreased ability to walk tion eventually.
h. Endocrine effects—menstrual irregularities, sterility in men
and women
(continued )](https://image.slidesharecdn.com/clinicaldrugtherapynursingcapituloonco-101007145706-phpapp02/75/Clinical-drug-therapy-nursing-capitulo-onco-20-2048.jpg)



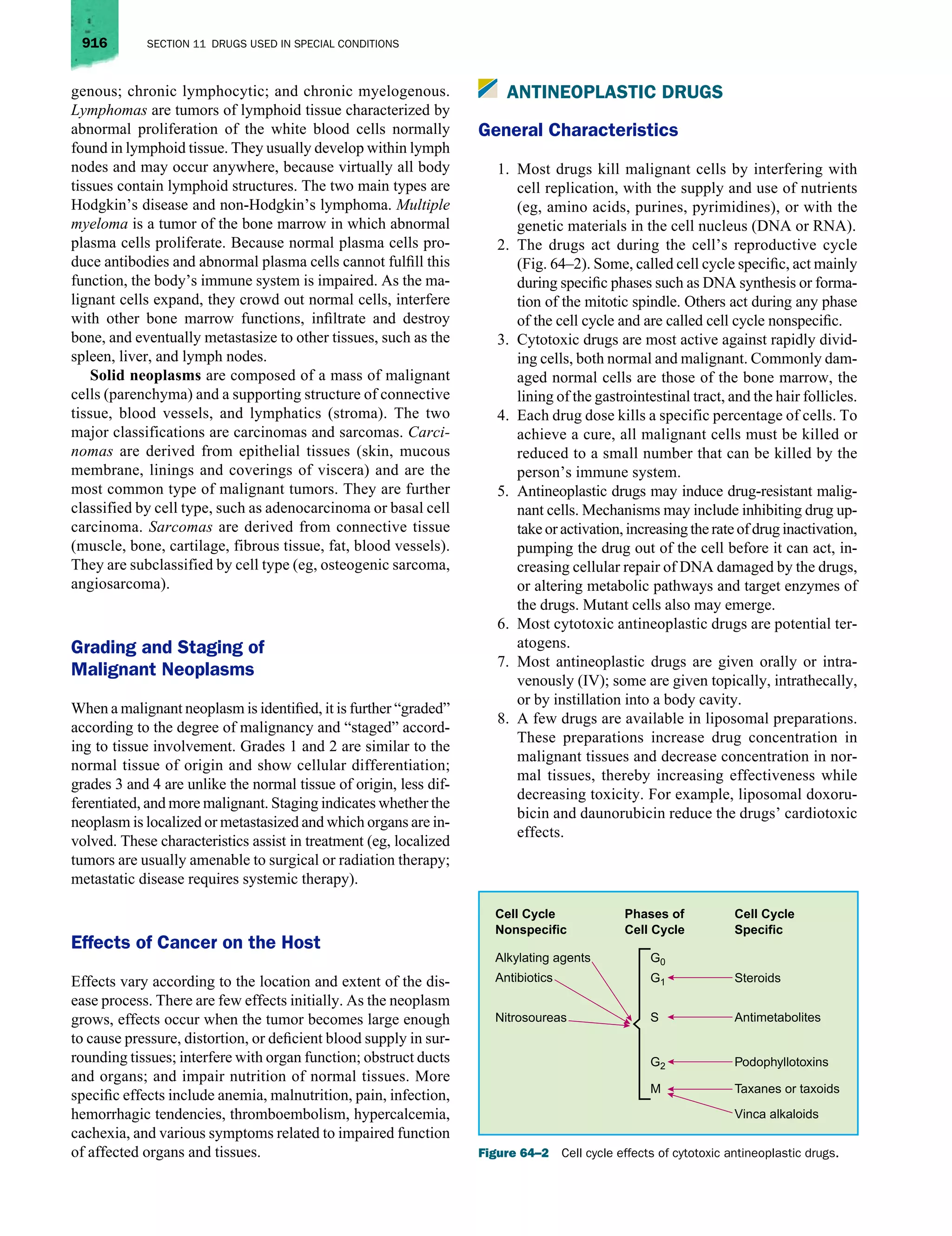
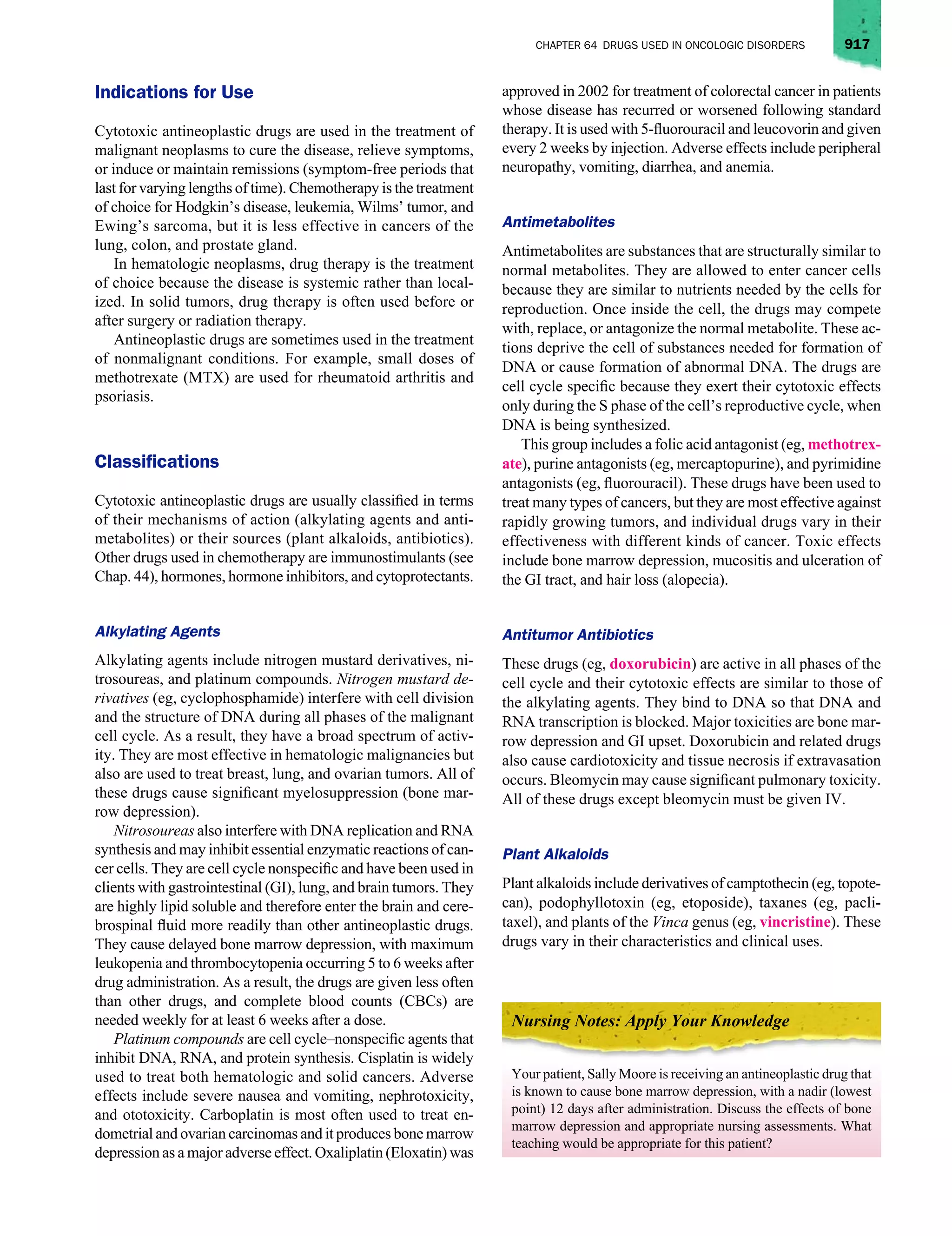
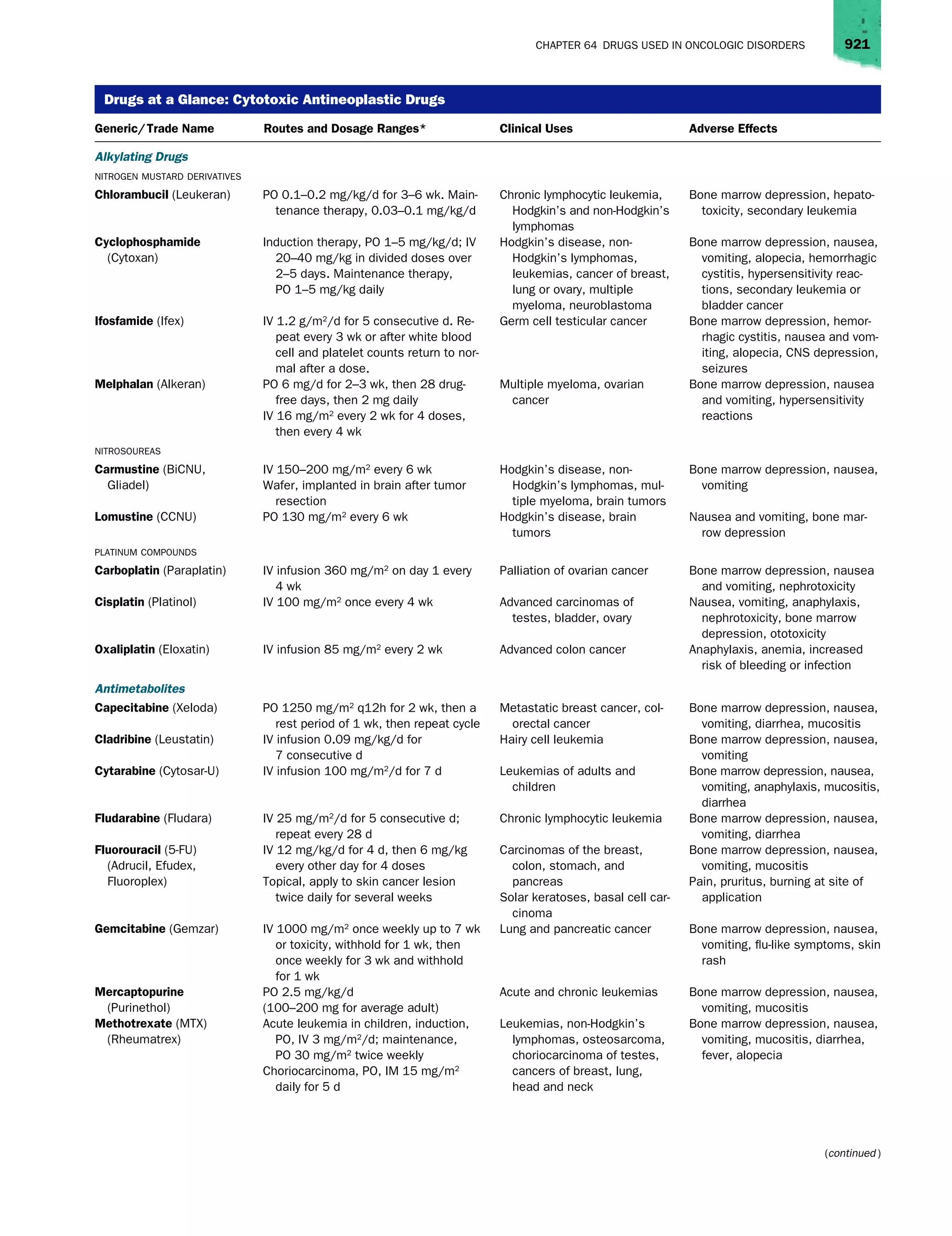
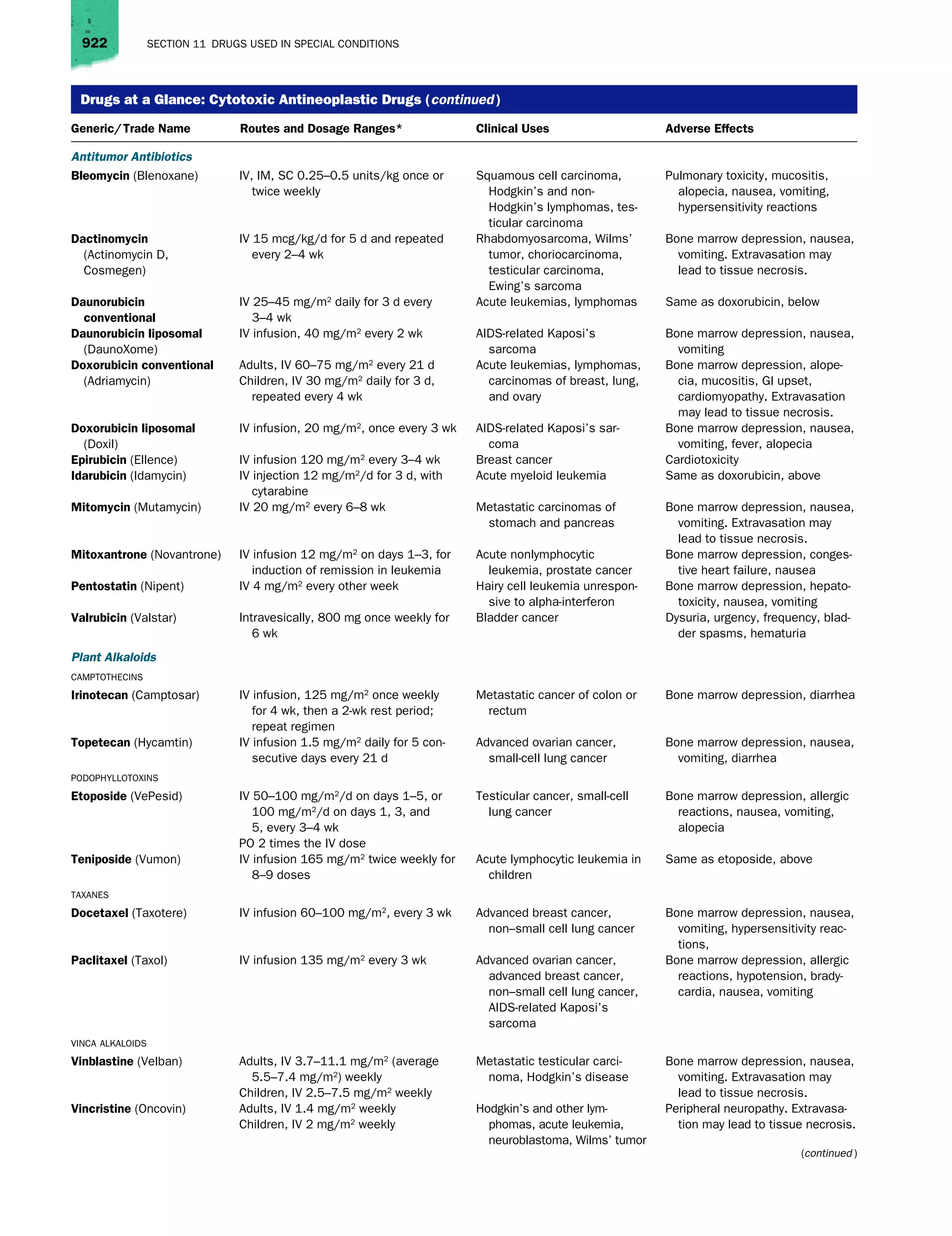
This document provides an overview of drugs used in oncologic disorders and chemotherapy. It contrasts normal and malignant cells, describing how cancer develops from genetic mutations that cause uncontrolled cell growth and proliferation. The major types of antineoplastic drugs are described in terms of their mechanisms of action, which generally interfere with cell replication or the genetic material in cancer cells. Combination chemotherapy using multiple drugs is discussed, along with managing the adverse effects of treatment.






























![Nutricion oncologicos[1]](https://cdn.slidesharecdn.com/ss_thumbnails/nutriciononcologicos1-111014153745-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)







































![Capacitacion nutricional corregida[1]](https://cdn.slidesharecdn.com/ss_thumbnails/capacitacionnutricionalcorregida1-111014153646-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)




