Downloaded 16 times


![clinicaloptions.com/oncology
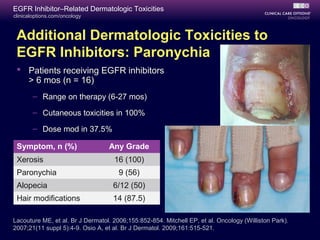
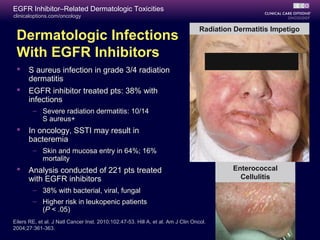
EGFR Inhibitor–Related Dermatologic Toxicities
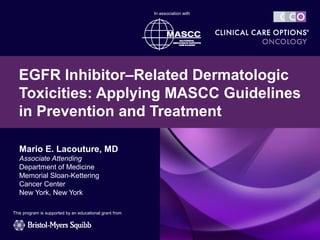
EGFR Inhibitor–
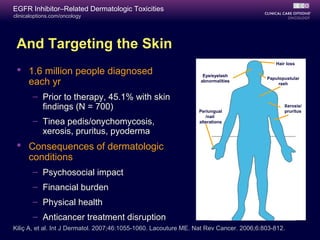
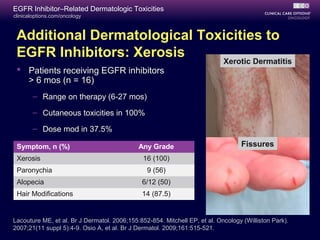
Induced Rash
Red papulopustules[1]
– Pruritus, tenderness in 62%
Erlotinib 150 mg QD[2]
– All grade: 75%
– Grade 3: 9%
Cetuximab[3]
– All grade: 85%
– Grade 3: 10%
Panitumumab[4]
– All grade: 90%
– Grade 3: 16%
Lapatinib[5]
– All grade: 27%
– Grade 3: 1%
1. Lacouture ME, et al. Br J Dermatol. 2006;155:852-854.
2. Shepherd FA, et al. N Engl J Med. 2005; 353:123-132.
3. Rosell R, et al. Ann Oncol. 2008;19:362-369.
4. Van Cutsem E, et al. J Clin Oncol. 2007;25:1658-1664.
5. Geyer CE, et al. N Engl J Med. 2006;355:2733-2743.](https://image.slidesharecdn.com/ccoegfrtoxicities2012slides-180407002419/85/Cco-egfr-toxicities_2012_slides-10-320.jpg)
![clinicaloptions.com/oncology
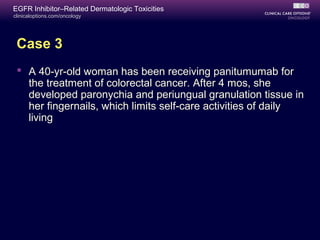
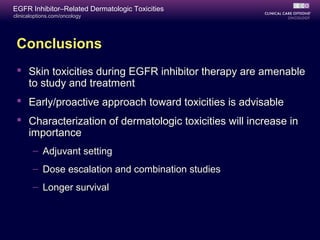
EGFR Inhibitor–Related Dermatologic Toxicities
1. Lacouture ME, et al. Br J Dermatol. 2006;155:852-854.
2. Shepherd FA, et al. N Engl J Med. 2005; 353:123-132.
3. Rosell R, et al. Ann Oncol. 2008;19:362-369.
4. Van Cutsem E, et al. J Clin Oncol. 2007;25:1658-1664.
5. Geyer CE, et al. N Engl J Med. 2006;355:2733-2743.
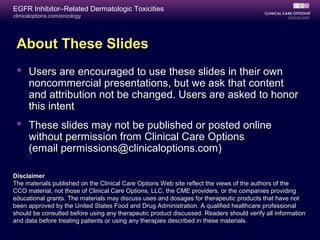
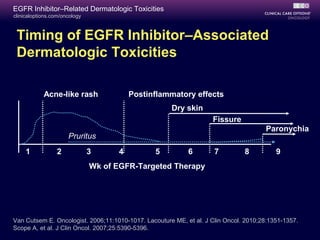
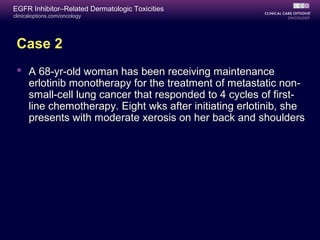
EGFR Inhibitor–
Induced Rash
Red papulopustules[1]
– Pruritus, tenderness in 62%
Erlotinib 150 mg QD[2]
– All grade: 75%
– Grade 3: 9%
Cetuximab[3]
– All grade: 85%
– Grade 3: 10%
Panitumumab[4]
– All grade: 90%
– Grade 3: 16%
Lapatinib[5]
– All grade: 27%
– Grade 3: 1%](https://image.slidesharecdn.com/ccoegfrtoxicities2012slides-180407002419/85/Cco-egfr-toxicities_2012_slides-11-320.jpg)
![clinicaloptions.com/oncology
EGFR Inhibitor–Related Dermatologic Toxicities
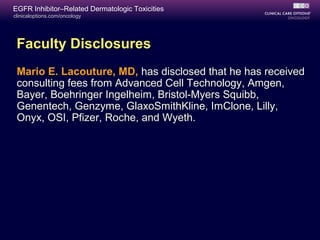
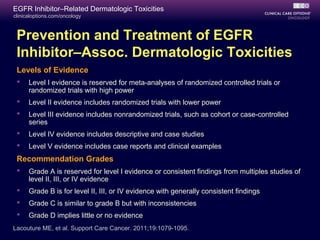
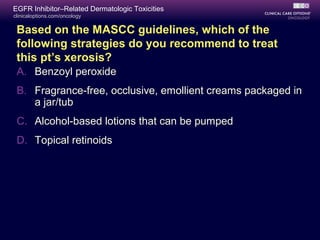
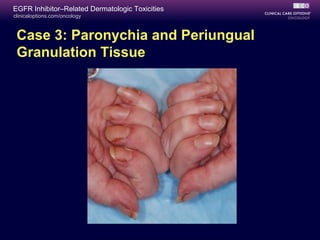
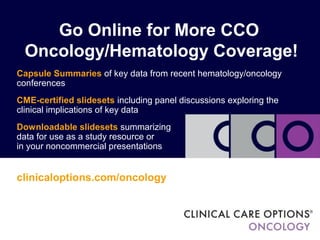
QoL[1]
Cost[2]
Impact of EGFR Inhibitor Dermatologic
Toxicities on QoL and Cost
Survey of 58 patients with Skindex-16
Top domain: emotions (P < .05)
Inverse corr age-emotions (r = -0.26; P = .03)
Mean cost/pt: $2788
MedianOverall
Skindex-16Score
NCI-CTCAE v3.0 Papulopustular Rash Grade
100
40
80
60
20
0
1 2 3
Drugs
Clinic Visits
Lab Tests
Procedures
1. Joshi SS, et al. Cancer. 2010;116:3916-3923. 2. Borovicka JH, et al. ASCO 2010. Abstract 3569.
Avg.Cost/PtforManagementofEGFR
InhibitorDermatologicToxicities($)
1497
862
338
91
0
200
400
600
800
1000
1200
1400
1600](https://image.slidesharecdn.com/ccoegfrtoxicities2012slides-180407002419/85/Cco-egfr-toxicities_2012_slides-12-320.jpg)
![clinicaloptions.com/oncology
EGFR Inhibitor–Related Dermatologic Toxicities
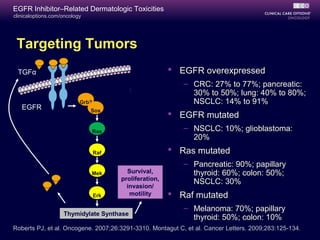
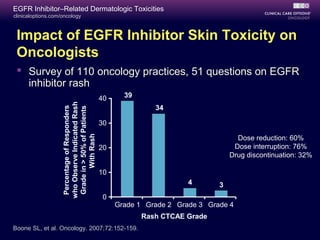
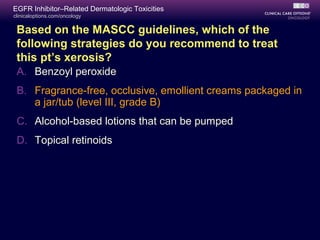
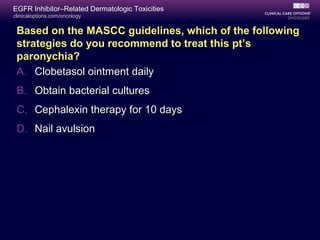
Vincenzi 2006[1]
P = .06
Saltz 2004[2]
P = .02
Hecht 2007[3]
HR: 0.72; 95% CI: 0.54-0.97
Grade 0-1
Grade 2-4
Grades 0-2
Grade 3
Grade 0
Grade 3
Median OS (Mos)
0 5 10
Cetuximab
Cetuximab
Panitumumab
RashGrade
Correlation: Rash and Survival/Response
in CRC
1. Vincenzi B, et al. Br J Cancer. 2006;94:792-797. 2. Saltz LB, et al. J Clin Oncol. 2004;22:1201-1208.
3. Hecht JR, et al. Cancer. 2007;110:980-988.](https://image.slidesharecdn.com/ccoegfrtoxicities2012slides-180407002419/85/Cco-egfr-toxicities_2012_slides-14-320.jpg)
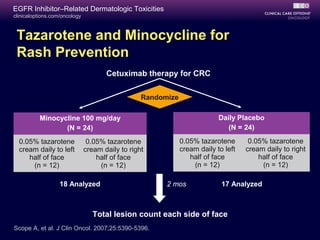
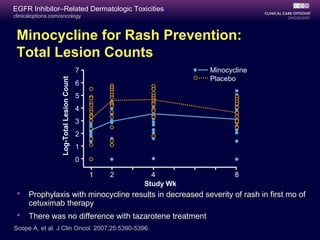
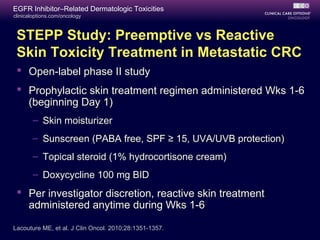
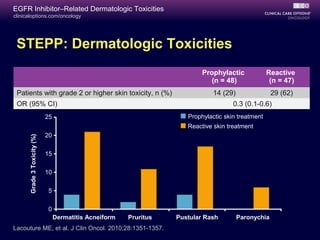
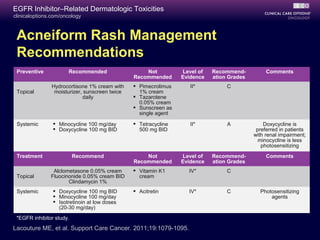


The document discusses guidelines for preventing and treating dermatologic toxicities caused by EGFR inhibitor therapies, noting that a rash occurs in the majority of patients and can impact quality of life. It recommends systemic minocycline or doxycycline during the first 1-6 weeks of EGFR inhibitor therapy to prevent acneiform rash based on level II evidence with a grade A recommendation. Topical hydrocortisone cream with sunscreen and moisturizer is also recommended to prevent and treat rash.
















































![Nutricion oncologicos[1]](https://cdn.slidesharecdn.com/ss_thumbnails/nutriciononcologicos1-111014153745-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)


![Capacitacion nutricional corregida[1]](https://cdn.slidesharecdn.com/ss_thumbnails/capacitacionnutricionalcorregida1-111014153646-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)



































