Download as PDF, PPTX


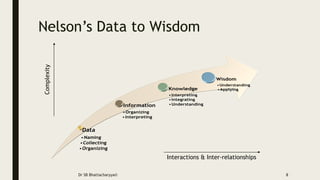








The document discusses the evolution and importance of clinical data analytics in healthcare, highlighting the transition from historical medical practices to modern empirical approaches. It elaborates on the methods of data collection, analysis, and interpretation, including the necessity of understanding statistics in clinical settings. The content also emphasizes the role of big data and machine learning in enhancing decision-making and patient care outcomes.









































![[Typ]Presentation[Sbj]LaboratoryDiagnosisDefined[Dte]20131028](https://cdn.slidesharecdn.com/ss_thumbnails/fe301b5e-1fa1-4d1a-8897-b1769d62f289-160502193918-thumbnail.jpg?width=640&height=640&fit=bounds)



































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)



