Downloaded 98 times
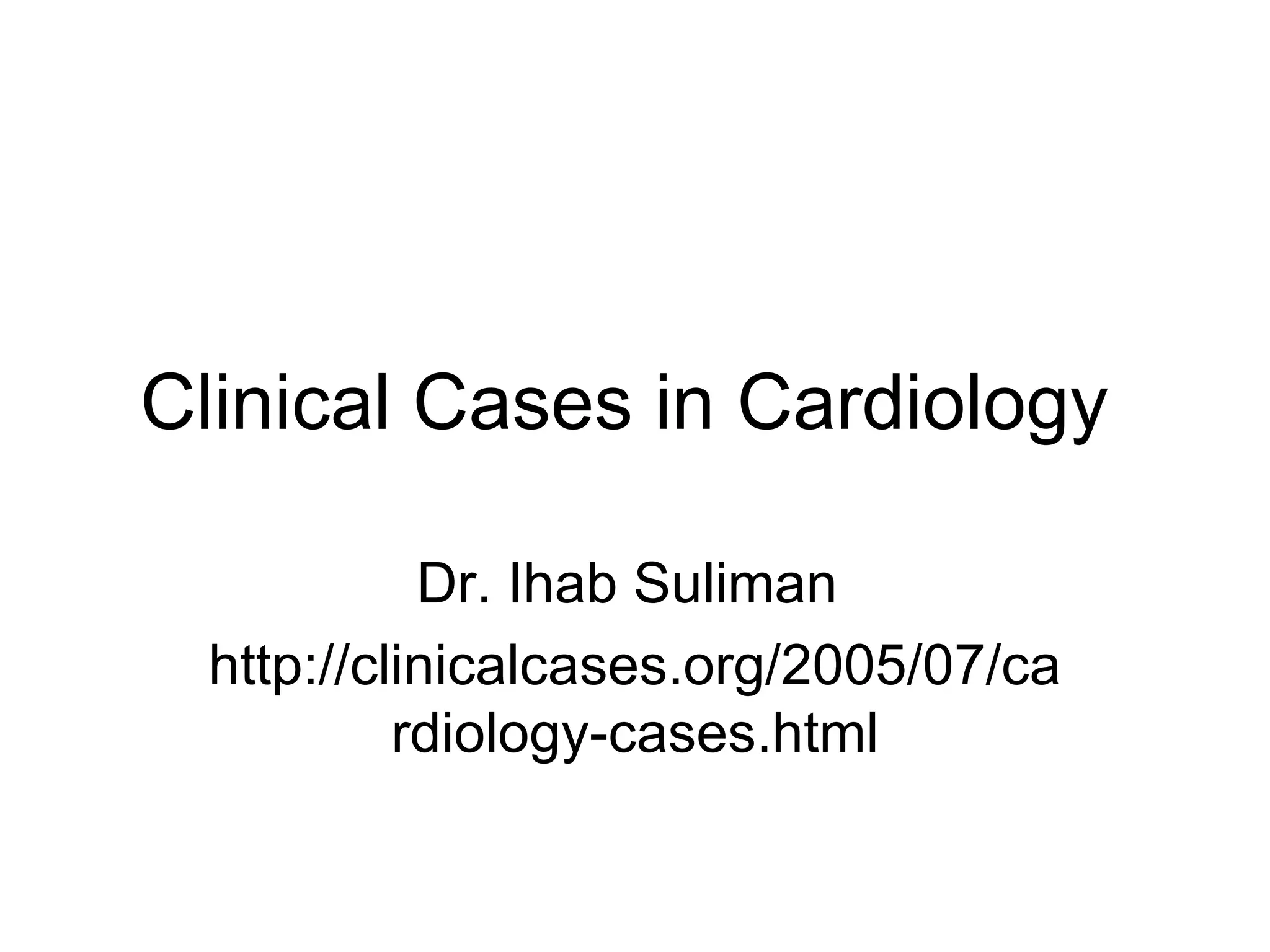
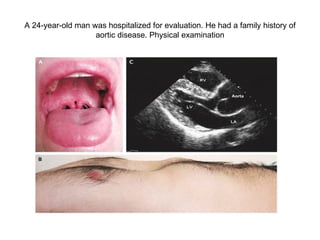
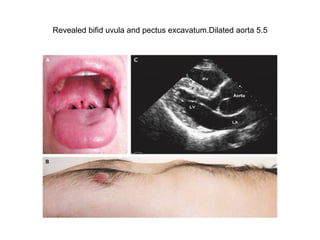

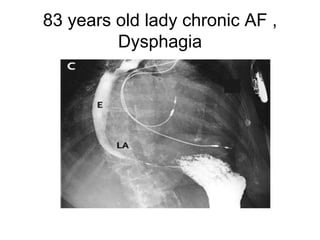

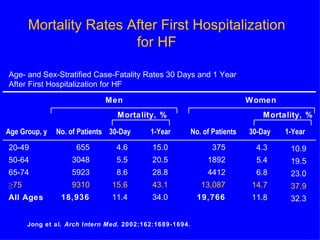




A 24-year-old man was hospitalized for evaluation of a dilated aorta and was diagnosed with Loeys-Dietz syndrome type 1 based on genetic analysis showing a mutation. An 83-year-old woman with atrial fibrillation and pacemaker presented with heart failure symptoms. Mortality rates after first hospitalization for heart failure are higher in men and increase with age.
























































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)


![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)













