Downloaded 111 times
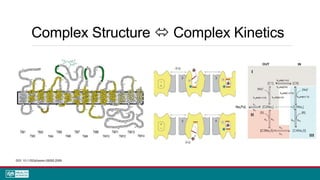
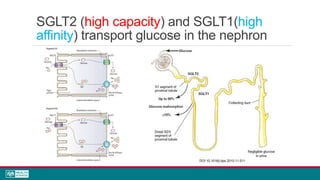
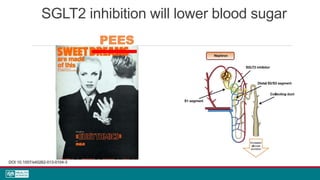
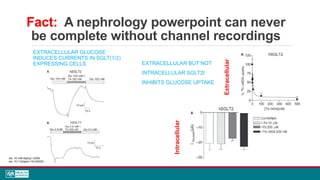
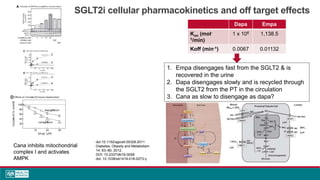
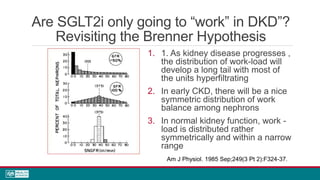

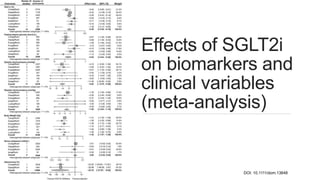
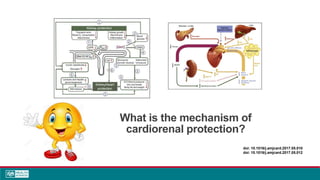
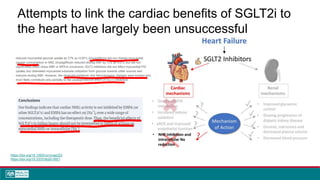
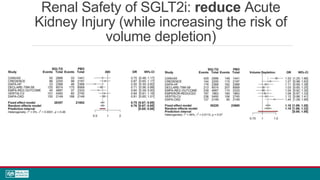
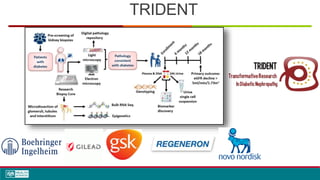


This document discusses sodium glucose cotransporter-2 inhibitors (SGLT2i) across the spectrum of renal diseases. It begins with an overview of renal glucose handling and the role of the SGLT2 channel. It then reviews the rationale for SGLT2 inhibition in diabetic and non-diabetic kidney diseases and basic SGLT2i pharmacology. Finally, it examines clinical outcomes data from trials demonstrating the cardiovascular, renal, and heart failure benefits of SGLT2is across levels of renal function and in diabetic and non-diabetic patients.








































































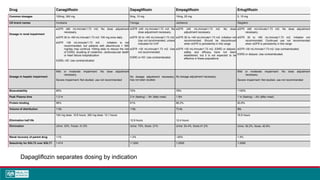
![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)













