Downloaded 14 times


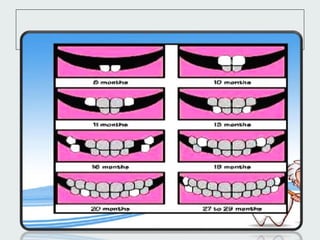
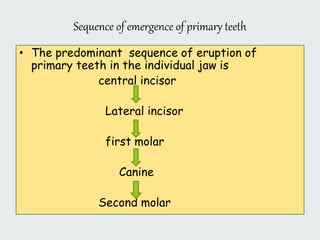
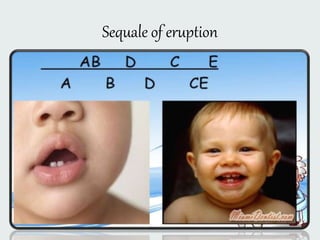
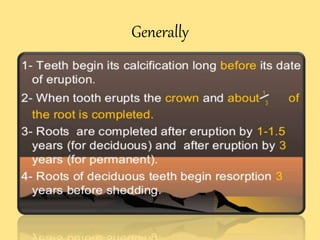
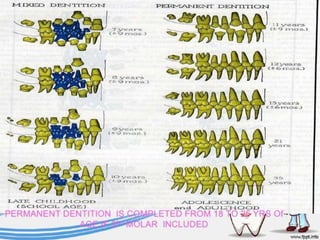

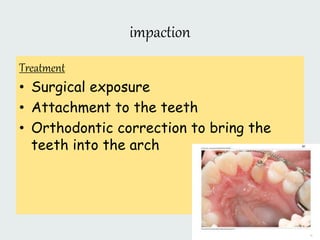

This document discusses dental anatomy and histology, specifically focusing on tooth eruption. It begins with an introduction and overview of the mechanisms and chronology of eruption. It then discusses the sequence of emergence for primary and permanent teeth. Potential disorders of eruption are also reviewed, including impaction caused by obstacles like supernumerary teeth, odontomas, or arch length deficiencies. Treatment options for various eruption disorders include surgical exposure, attachment of impacted teeth for orthodontic alignment, and removal of hard tissue obstacles blocking eruption.













![[Pedo] restorative dentistry](https://cdn.slidesharecdn.com/ss_thumbnails/pedorestorativedentistry-210903140140-thumbnail.jpg?width=640&height=640&fit=bounds)

![[Crown & Bridges] [terminology & classification]](https://cdn.slidesharecdn.com/ss_thumbnails/lec01-02terminologyclassification-151105130852-lva1-app6892-thumbnail.jpg?width=640&height=640&fit=bounds)

























































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)






