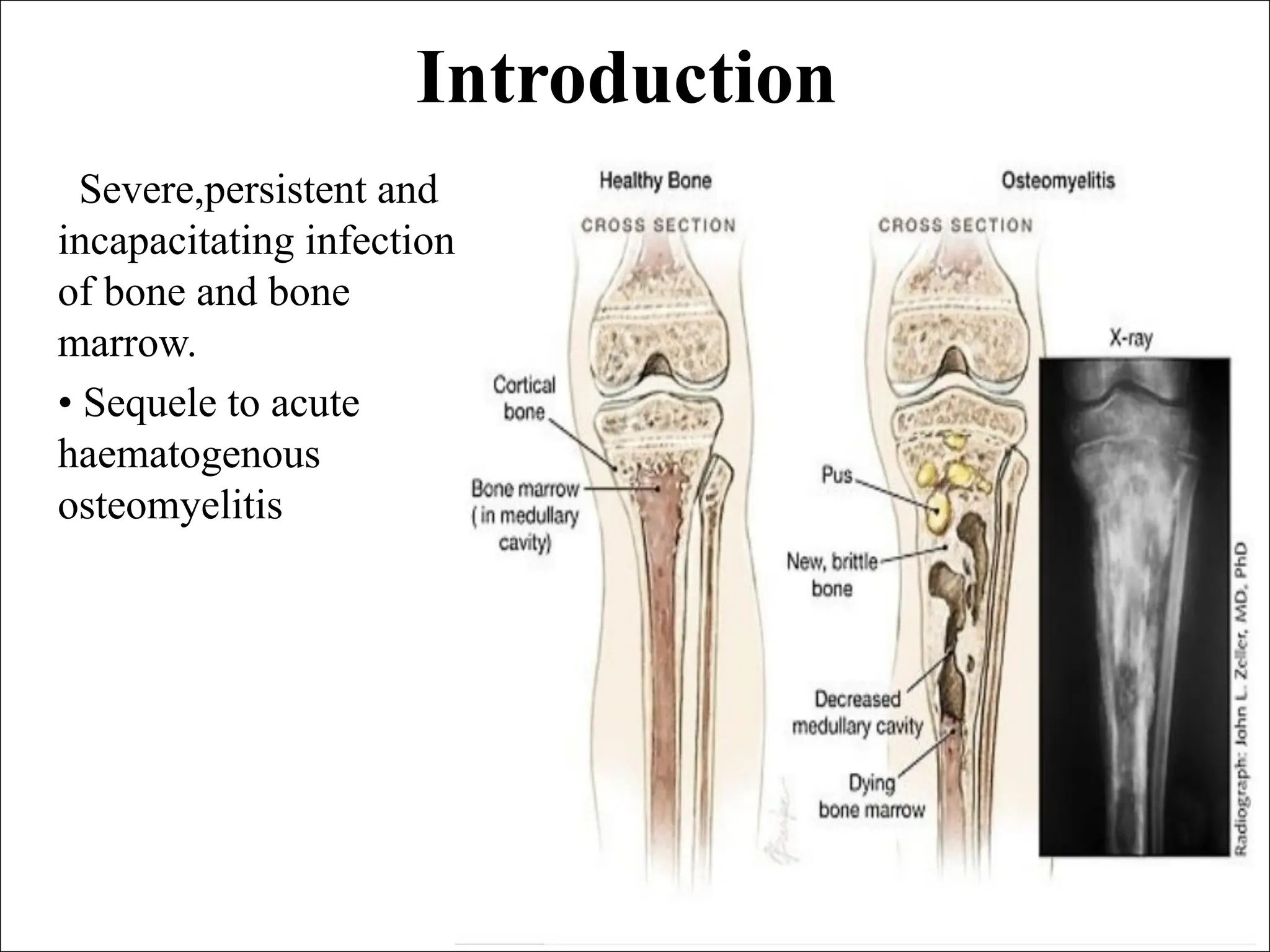
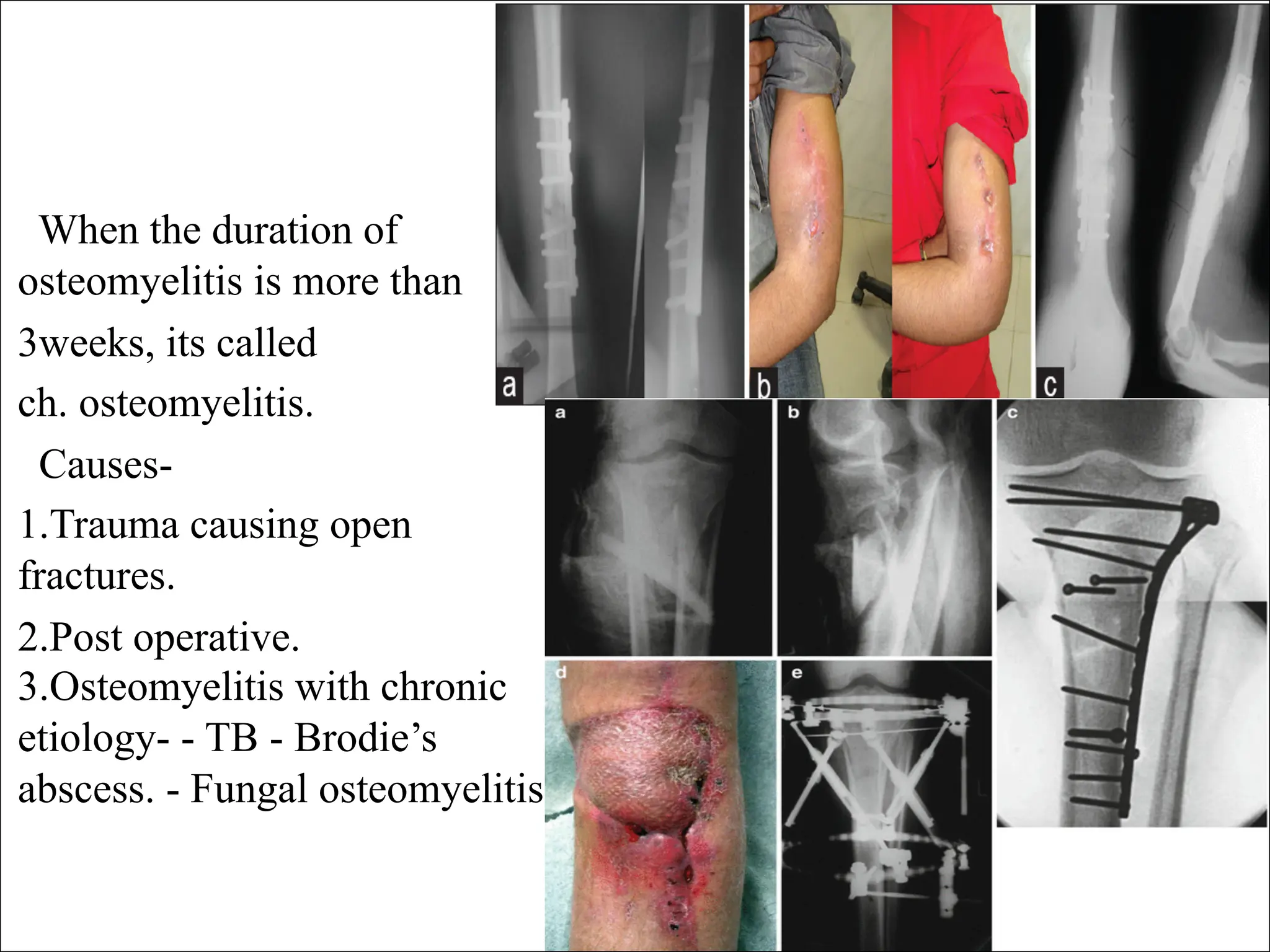
Chronic osteomyelitis is a severe, persistent infection of bone resulting from various causes, including trauma and postoperative complications. It is characterized by necrotic bone, purulent material, and an avascular envelope that renders systemic antibiotics largely ineffective. Diagnosis involves clinical examination and imaging studies, while treatment often requires surgical intervention followed by a course of intravenous antibiotics.















![Treatment
Supportive treatment .
Antibiotics – to prevent
spread.
Surgery – sequestretomy +
saucerization [cannot be
eradicated without surgical
intervention]
Sinus tracks can be injected
with methylene blue 24 hours
before surgery to make them
easier to locate and excise.](https://image.slidesharecdn.com/chronicosteomyelitis2-240716132925-609579d2/75/Chronic-osteomy-lllhhhhhhhhhhhhhhhhelitis-2-pdf-18-2048.jpg)








































































