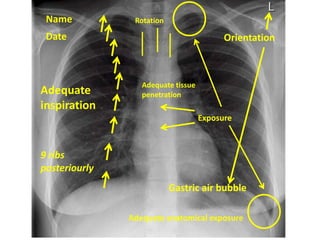
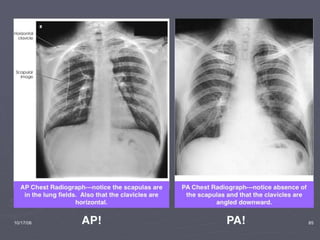
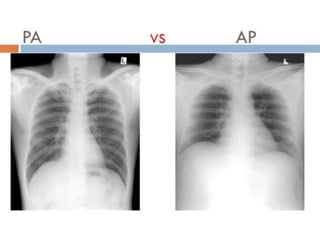
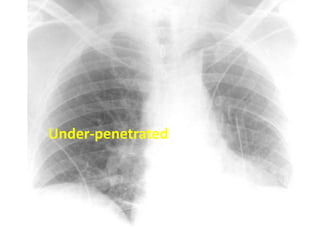
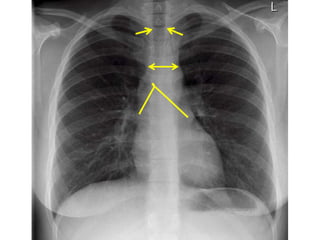
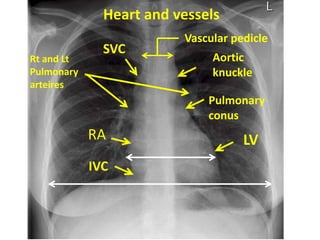
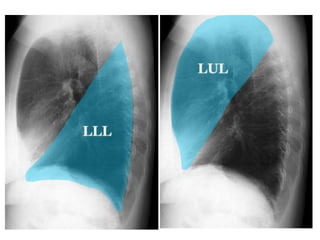
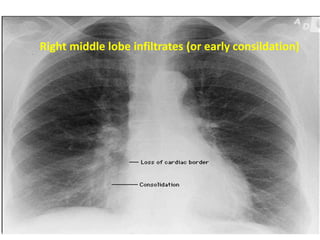
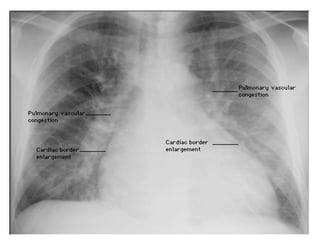
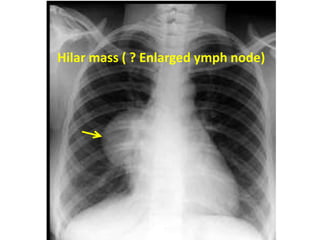
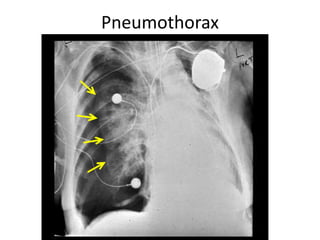
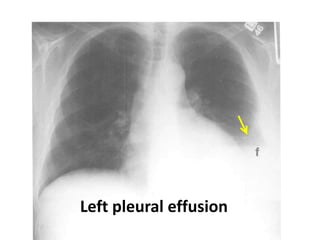
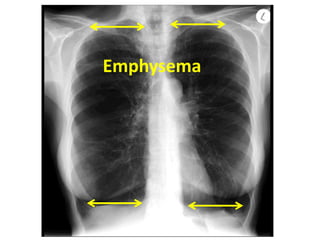
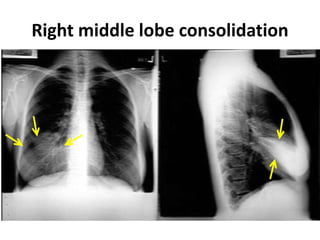
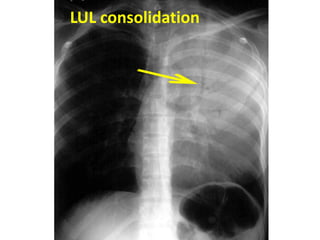
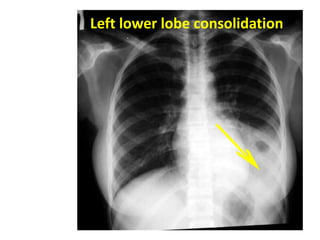
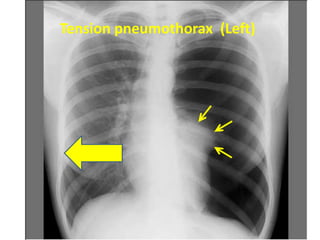
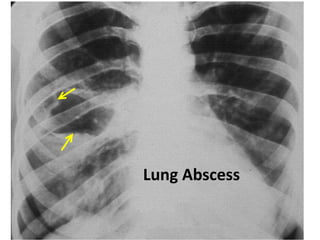
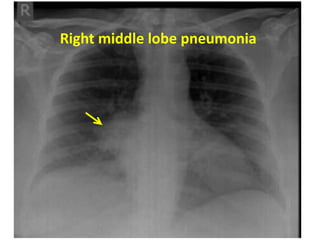
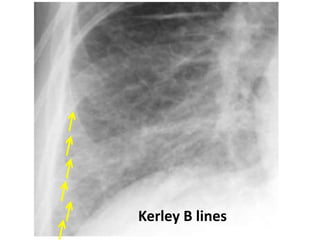
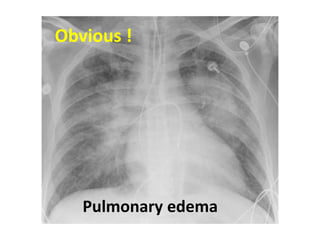
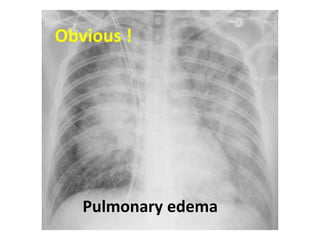
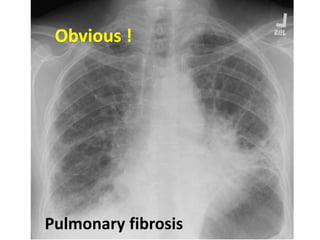
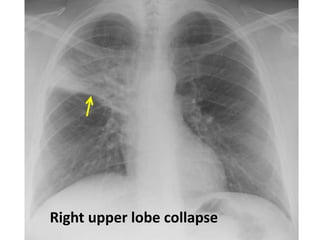
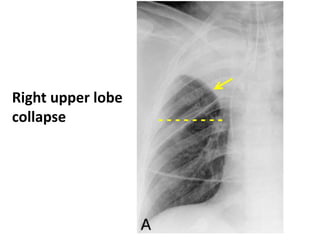
This document provides a systematic approach to interpreting chest X-rays, emphasizing the importance of verifying patient details, orientation, and adequate exposure. It outlines key areas to inspect including the trachea, heart, diaphragm, lung fields, and bones while identifying potential abnormalities such as pneumonia, effusions, and masses. The interpretation guide stresses the examination of various specific features like the angle of the carina, mediastinum width, and pulmonary structures, aiming for thorough diagnostic evaluations.