Download to read offline
![Little, D. [DrDLittle]. (2013, December 17). [Tweet]. Retrieved https://twitter.com/DrDLittle/status/412998428755767296
We should probably CT it anyway to make sure its a duck
If it walks like a duck… and swims like a duck… and quacks like a duck…](https://image.slidesharecdn.com/2017aapa-madaykr-toimageornottoimage-noarsquestions-170531143943/85/Radiographic-Decision-Making-3-320.jpg)

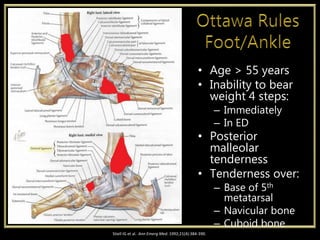
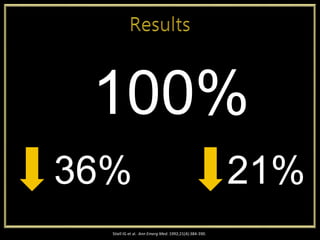
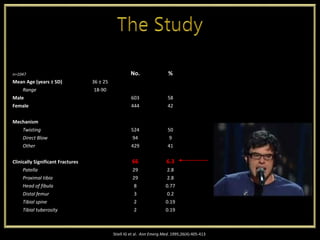
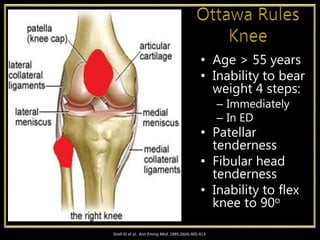


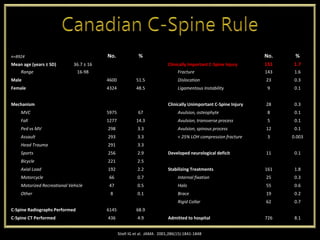
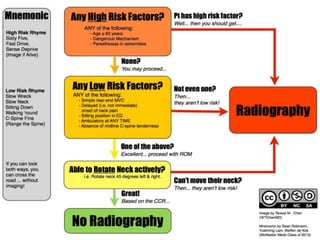
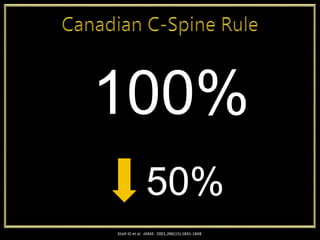
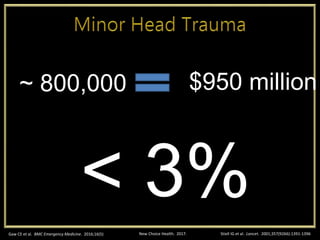
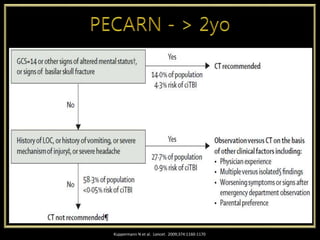
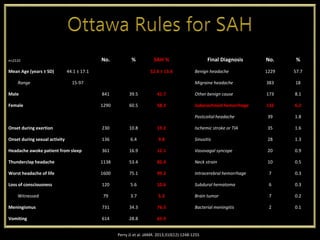



This document provides a summary of several clinical decision rules and guidelines used in emergency medicine to determine the need for imaging or other diagnostic tests. It discusses rules for ankle/foot fractures, knee fractures, cervical spine injuries, minor head injuries, and subarachnoid hemorrhage. For each rule, it provides the essential criteria included in the rule as well as validation studies showing the sensitivity and specificity of the rules. The overall message is that these clinical decision rules can help standardize clinical decision making and reduce unnecessary testing, but clinicians must first thoroughly evaluate the patient's history and presentation before applying any rule.












































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)


![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)

