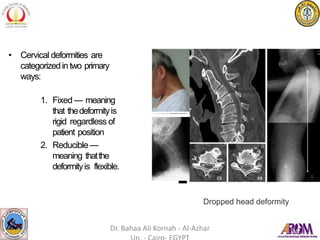
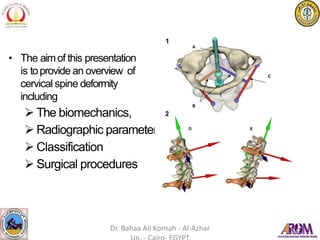
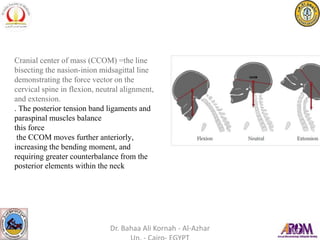
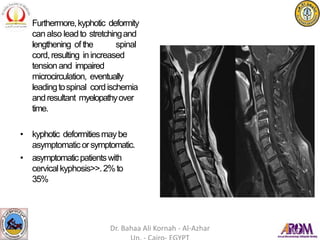
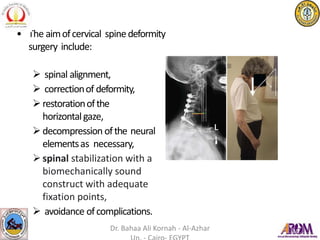
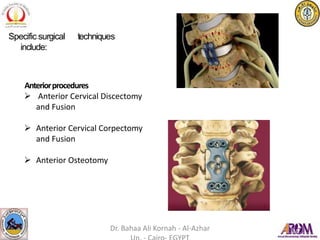
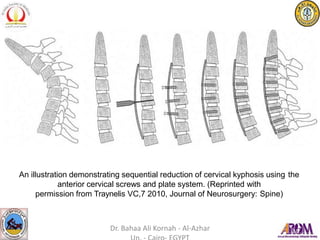
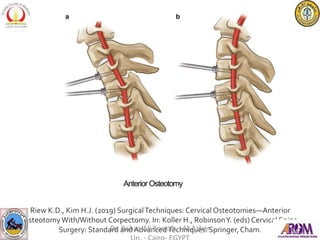
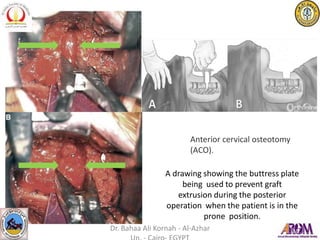
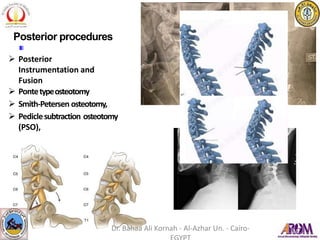
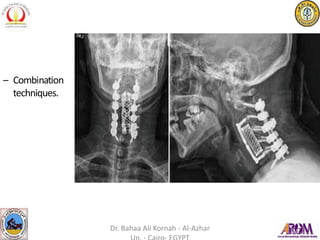
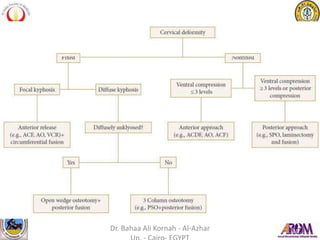
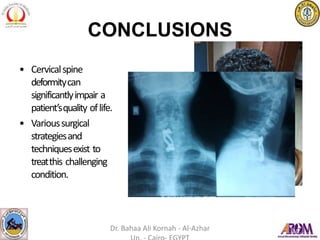
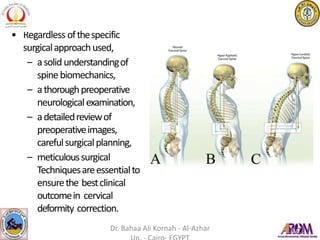
The document discusses cervical spine deformities, their impact on quality of life, common causes, and characteristics. It describes the biomechanics, classification systems, and various surgical procedures available for correction, emphasizing the importance of spinal alignment and decompression of neural elements. The presentation underscores the need for thorough preoperative evaluation and meticulous surgical techniques to achieve optimal outcomes.


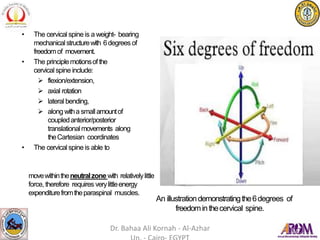

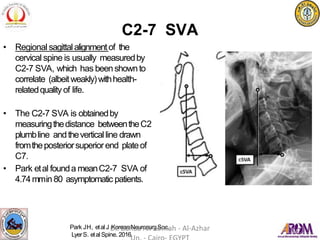











![PFFD [proximal femoral focal deficiency]](https://cdn.slidesharecdn.com/ss_thumbnails/pffdproximalfemoralfocaldeficiency-200421181838-thumbnail.jpg?width=640&height=640&fit=bounds)












































































