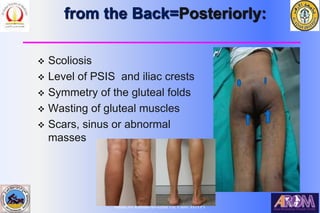
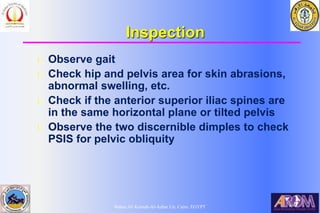
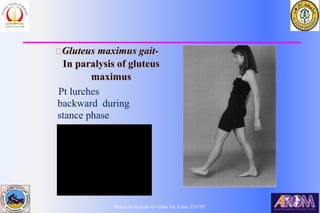
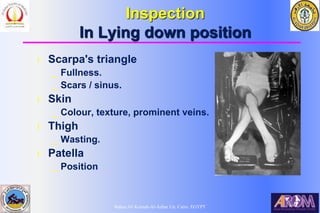
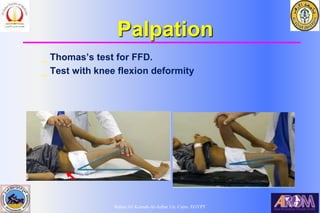
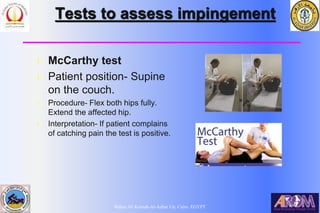
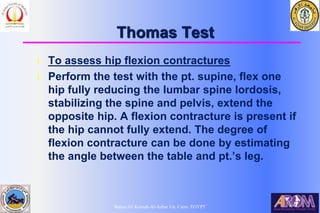
Dr. Bahaa Ali Kornah discusses the systematic approach to clinical hip examination, emphasizing the importance of a structured method in practice. Key components include thorough patient history regarding symptoms, functional capabilities, and examination techniques such as inspection and palpation. The document provides detailed insights on assessing various hip conditions through specific examinations and tests.