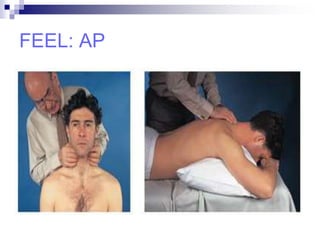
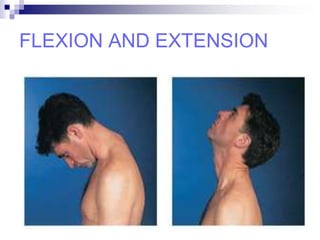
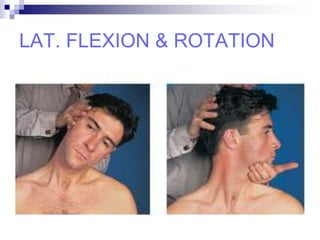
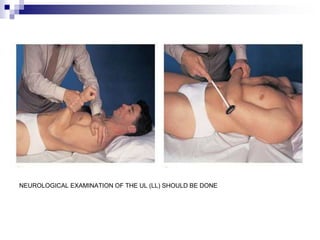
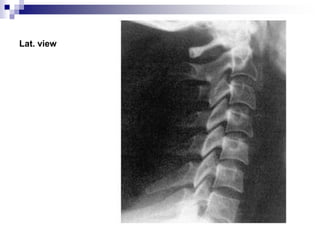
This document provides an overview of examining the neck and various neck deformities. It begins with a brief anatomy section covering the bones and structures of the neck. It then outlines the steps to examine the neck - looking at the neck from all angles, feeling the bony contours and muscles, and moving the neck through its range of motion. Various neck deformities are classified and described, including congenital torticollis, Klippel-Feil syndrome, congenital high scapula, and ankylosing spondylitis. Treatment options are mentioned for each condition. Special tests to evaluate neurological involvement are also outlined.