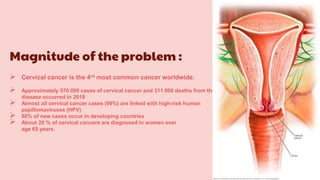
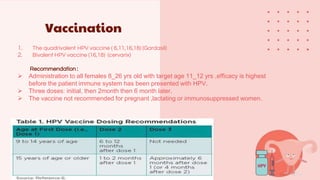
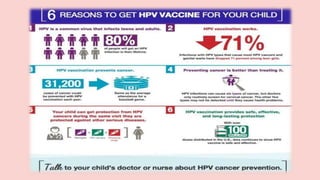
Cervical cancer is the fourth most common cancer globally, with approximately 570,000 cases and 311,000 deaths in 2018, predominantly affecting women in developing countries. Most cases are linked to high-risk HPV, and early diagnosis through procedures like Pap smears and colposcopy significantly reduces mortality rates. Prevention strategies include vaccination for girls aged 9–13, healthy sexual behavior education, and regular screenings to identify precancerous lesions.

















































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)

