Anatomy and Physiologyof the Cervix:
Important Terms
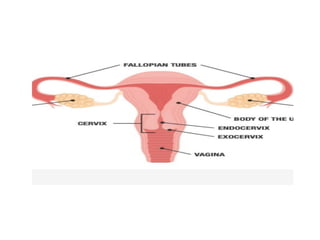
Cervix is lower part of uterus that connects to vagina
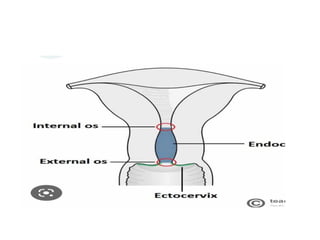
Exocervix: connects to vagina
The opening in the exocervix(external os) marks the transition from
the ectocervix to the endocervical canal
Covered with squamous epithelium
Endocervix: inner region of the cervix
Covered with glandular columnar epithelium
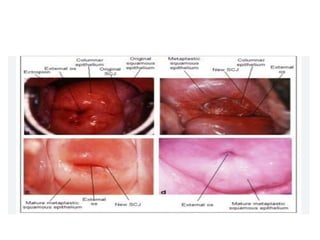
Squamocolumnar junction (SCJ)
Place where squamous cells meet columnar cells
Is usually visible on cervix as a line
5.
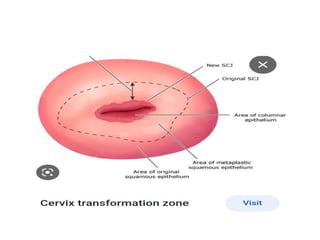
The SCJis dynamic and moves during early adolescence
and during first pregnancy
The original SCJ originates in the endocervical canal but as
the cervix everts during adolescence or pregnancy the SCJ
comes to lie on the ecto cervix and becomes the new SCJ.
The epithelium between these two SCJ is the transition
zone ,its position also is variable and is the site where
malignant transformation occurs.
TZ is more ectocervical during women's reproductive year
and return to endocervix during menopause
7.
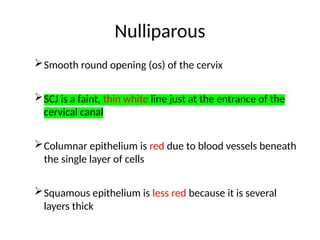
Nulliparous
Smooth round opening(os) of the cervix
SCJ is a faint, thin white line just at the entrance of the
cervical canal
Columnar epithelium is red due to blood vessels beneath
the single layer of cells
Squamous epithelium is less red because it is several
layers thick
8.
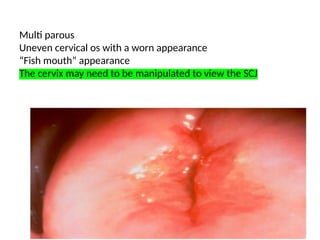
Multi parous
Uneven cervicalos with a worn appearance
“Fish mouth” appearance
The cervix may need to be manipulated to view the SCJ
Nulliparous
9.
Function of thecervix
Produce cervical mucus which block ascent of
pathogens
Facilitate passage of sperm in to uterine cavity
Canal for passage of menstrual flow
Canal for fetal passage to vagina during labor
by dilatation
10.
CIN
the termintraepithelial neoplasia refers to epithelial
lesions that are potential precursors of invasive cancer.
These lesions demonstrate a range of histologic
abnormality from mild to severe based on cytoplasm,
nuclear, and histologic changes.
The severity of squamous intraepithelial lesions is
graded by the proportion of epithelium with abnormal
cells.
These alterations begin at the basement membrane
and continue upward toward the epithelium surface.
11.
With cervical intraepithelialneoplasia (CIN), abnormal
cells solely confined to the lower third of the squamous
epithelium are referred to as mild dysplasia or CIN 1.
Those that extend into the middle third are moderate
dysplasia or CIN 2,· into the upper third, severe
dysplasia or CIN 3; and
full-thickness involvement, carcinoma in situ (CIS).
Preinvasive squamous lesions of the vagina, vulva,
perianal, and anal squamous epithelia are graded
similarly to CIN.
12.
Precancerous changes almostalways develop
in the T-zone and specifically on or near SCJ
Screening for precancerous lesions should
focus on the T-zone and SCJ because that is
where a dangerous lesion will develop
14.
Squamous metaplasia
Physiologic processthrough which the glandular cells
lining the cervical canal near the SCJ are replaced with
squamous cells
Due to cervix’s exposure to noxious agents in the
environment such as bacteria, viruses, and unclean
foreign bodies
Has a thin white, veil appearance that will not wipe
away
15.
Ectropion
also calledEctropy /cervical erosion
Condition where cell lining the inside of the cervix evert on to the
outside of the cervix
glandular cells mixed into the squamous cells, can extend onto vagina
continuously
normal, may reflect microglandular hyperplasia (benign, OCP)due to high
estrogen exposure
17.
Risk factors
Risk factorsfor CIN are similar to cervical cancer and
include the following
Demographic risk factors
Ethnicity (Latin American countries, U.S. minorities)
Low socioeconomic status
Increasing age
Behavioral risk factors
Early coitarche
Multiple sexual partners
Male partner with multiple prior sexual partners
Natural History
The naturalhistory of HPV infection include
Regression
Persistent infection
Progression to preinvasive lesion
Progression to invasive carcinoma from high grade
lesion
The risk of progression to invasive cancer rises with
CIN severity.
20.
Low grade lesionsare thought to be
manifestations of acute HPV infection, and
approximately 90 percent regress within a few
years.
High-grade lesions are less likely to regress.
Approximately 40% CIN 2 cases show
spontaneous regression within 2 years.
This is even more frequent (>60 percent) in
young, healthy women.
21.
CIN 2 isthought to be a mixture of low- and
high-grade lesions that are difficult to
distinguish histologically, rather than an
intermediate step in the progression from CIN
1 to CIN 3.
The risk of progression of biopsied but
untreated CIN 3 to invasive cancer
approximates 30 percent over 30 years.
22.
Prevention of cervicalcancer
1)Primary prevention
Involve primary prevention of HPV infection like
A)behavioral changes abstinence from sexual intercourse, being
mutually faithful in relation and consistent use of condoms
B) HPV vaccination which are found as
Cervarix (bivalent vaccine )that targets HPV 16&18
HPV Quadrivalent ( gardasil 4)that targets HPV 16,18 and low
risk serotypes HPV 6&11
HPV Nonavalent ( gardasil 9)that targets HPV
16,18,6,11,31,33,45,52 and 58
23.
HPV is recommendedto be give for all male and
female age 9-13 years old
For adolescents and adults aged13-26 who have not
been previously vaccinated or who have not
completed the vaccine series , catch-up vaccination
is recommended
For those above 27 years , catch-up vaccination is
not recommended but studies have shown that HPV
is safe and effective in those above 27 and in USA it
is give up to 45 years of age.
24.
Prior history ofsexual contact , abnormal pap status ,
genital wart or prior HPV infection is not
contraindication for vaccination.
Immunization schedule
For individual starting the vaccine at 9-14 years of
age, two dose of HPV should be give at 0&6 to 12
month interval
For individual starting the vaccine at 15 years or
older ,three doses given at 0,2 months and 6 months
25.
Minimum intervalbetween the doses is at least 4 weeks between the first
two doses and 12 weeks between the second and third dose and 5
months between the first and third dose.
If a dose was administered at a shorter interval ,it should be repeated
once the minimum recommended interval since the most recent dose has
passed
26.
Immunocompromised patients -three doses of HPV
vaccine should be given at 0,2month and 6 month
interval regardless of age.
Missed doses-the ACIP recommends that if the
vaccination series is interrupted for any length of time ,
it can be resumed without restarting the series.
HPV vaccination is not recommended during pregnancy
because of limited information on its safety during
pregnancy but can be given for lactating women
27.
Efficacy varies forthe vaccine types and generally
range from 99%in HPV naïve to 44-61% in overall
population in preventing CIN -2 and above and
CIS.
2)Secondary prevention
halts the progression of the diseases once it has
started.
Includes screening and treatment of
precancerous cervical lesion
28.
CERVICAL INTRAEPITHELIAL NEOPLASIADIAGNOSIS
Cytology(Pap smear)
HPV DNA test
Co-test
Resource limited set up
VIA
VILI
NB:Read on how each tests are done and interpretation
29.
Current Cervical CancerScreening Guideline
Screening Initiation
Cervical cancer screening begins at age 21 in average-risk women.
This is true regardless of sexual history, sexual orientation, or other
risk factors.
Screening Strategies and Intervals
For women aged 21 to 29 years, all current guidelines recommend
screening with cytology alone at 3-year intervals.
Women aged 30 to 65 years can continue screening with cytology
alone at 3-year intervals or can begin co-testing at 5-year intervals
HPV DNA is incorporated by the WHO as primary screening
modality
30.
Screening Discontinuation
Screening maybe stopped at age 65 years in those at
average risk for cervical cancer and who have
undergone adequate screening, regardless of past or
current sexual history.
Adequate screening is defined as three consecutive,
negative cytology results or two consecutive,
negative co-test results in the prior 10 years, with
the most recent result occurring within the past 5
years.
31.
Women withprior treatment for CIN 2, CIN 3, AIS, or
cervical cancer should continue screening for at least 20
years past their diagnosis and treatment, even if this
extends screening beyond age 65.
Post hysterectomy
Primary vaginal carcinoma is rare and makes up < 5
percent of all gynecologic malignancies .
All guidelines recommend against Pap test screening for
women who have undergone total hysterectomy (cervix
removed) for a benign disease indication and who lack a
prior high-grade CIN or cervical cancer diagnosis
32.
lmmunocompromised Patients
WithHIV infection, screening should commence within 1 year of
sexual activity onset and no later than age 21 years.
Women aged 21 to 29 years should receive Pap testing at the time
of HIV diagnosis.
If an initial Pap test result is negative, testing should be repeated
6 or 12 months later and then continued every 12 months.
After three consecutive, negative Pap test results, the interval of
Pap testing can be extended to 3 years.
Cervical cancer screening is continued indefinitely even in those
aged 65 years or older who have been adequately screened.
33.
Colposcopy -is amagnified view of the
cervix , vaginal and vulva .
Indications
Unexplained lower genital tract bleeding
Abnormal cytology on pap
smear(LSIL,HSIL,ASC-H,AGC..)
Abnormal vaginal discharge
Grossly visible cervical lesion
34.
Management of CIN
1)Ablation
This involves physical destruction of tissue and is generally
effective for noninvasive ectocervical disease.
Commonly indicated for persistent CIN I and CIN 2
The most commonly used ablative treatment modalities are
cryosurgery , thermal ablation and carbon dioxide (CO2)
laser ablation
Ablation should not be used after previous therapy, after
glandular cytologic abnormalities, or for AIS and high grade
lesions.
35.
2) Excisional therapy
commonly used for high grade lesion(CIN-III, glandular
cytologic abnormalities, or for AIS and repeat therapy)
Includes LEEP(loop electrosurgical excision procedure)
and clod knife conization(CKC).
3) Hysterectomy is unacceptable as primary therapy for CIN
However, it may be considered when treating recurrent
high-grade cervical disease if childbearing has been
completed or if a repeat cervical excision is strongly
indicated but not technically feasible.
36.
3) Tertiary carefor cervical cancer
Care give once a women is diagnosed with
invasive cervical cancer
include surgery,radiotheraphy,chemotheraphy
and palliative care
37.
Cervical cancer
Cervical canceris the most common
gynecologic cancer in women worldwide.
Most of these cancers (99.7%) stem from
infection with the human papillomavirus (HPV)
Most early cancers are asymptomatic.
Thus, diagnosis usually follows histologic
evaluation of biopsies taken during colposcopic
examination or from a grossly abnormal cervix
38.
Fourth most commoncancer among women
world wide
569,847 new case and 311,000 death annually
In LMIC including Ethiopia commonest
reproductive organ cancer and leading cause of
death from cancer
In Ethipian,second most common cancer with
6200 new cases yearly with mortality close to
5000
39.
Cervical cancer ispotentially preventable diseases as
effective screening program led to significant
decrement in mortality and morbidity from cervical
cancer in developed countries.
Ethiopia launched the first ever national guideline on
cervical cancer screening and treatment in 2015
which served for 5 years
During the past 5 years, the national coverage of
cervical cancer screening and treatment for women
age 30-49 is only 5%.
40.
Human Papillomavirus Infection
This virus is the primary etiologic infectious agent associated
with cervical cancer.
Although other sexually transmitted factors, including herpes
simplex virus 2, may play a concurrent causative role,
99.7 percent of cervical cancers are associated with an oncogenic
HPV subtype.
Low risk HPV Types 6 & 11 associated with development of
genital warts
High risk types -16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, 59,
66 associated with development of dysplasia/cancer
41.
Each of theseserotypes can lead to either
squamous cell carcinoma or adenocarcinoma
of the cervix.
However, HPV 16 is more commonly
associated with squamous cell carcinoma of
the cervix, whereas HPV 18 is a risk factor for
adenocarcinoma of the cervix.
42.
PATHOPHYSIOLOGY
Tumorigenesis
Squamouscell carcinoma of the cervix typically arises at the
squamocolumnar junction from a preexisting dysplastic lesion, which
in most cases follows infection with HPV.
Although most women readily clear HPV, those with persistent infection
may develop preinvasive dysplastic cervical disease.
In general, progression from dysplasia to invasive cancer requires
several years, but wide variation exists.
The molecular alterations involved with cervical carcinogenesis are
complex and not fully understood.
Accordingly, carcinogenesis is suspected to result from the interactive
effects between environmental insults, host immunity, and somatic-cell
genomic variations.
43.
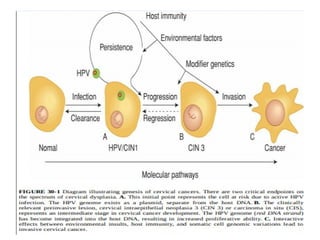
HPV playsa major role in the development of cervical cancers.
Increasing evidence also suggests that HPV oncoproteins may be
a critical component of continued cancer cell proliferation.
Unlike low-risk sero-types, oncogenic HPV serotypes can integrate
into the human genome.
As a result, with infection, oncogenic HPV’s early replication
proteins E1 and E2 enable the virus to replicate within cervical
cells.
These proteins are expressed at high levels early in HPV
infection.
They can lead to cytologic changes detected as low-grade
squamous intraepithelial (LSIL) cytologic findings on Pap smears.
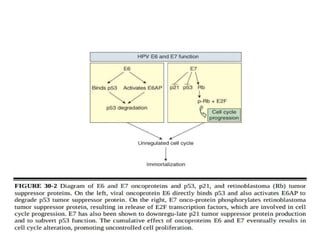
45.
Amplification ofviral replication and subsequent
transformation of normal cells into tumor cells may follow.
Specifically, viral gene products E6 and E7 oncoproteins
are implicated in this transformation.
E7 protein binds to the retinoblastoma (Rb) tumor
suppressor protein, whereas E6 binds to the p53 tumor
suppressor protein.
In both instances, binding leads to degradation of these
suppressor proteins.
The E6 effect of p53 degradation is well studied and linked
with the proliferation and immortalization of cervical cells.
47.
Tumor Spread
Following tumorigenesis,the pattern of local growth may
be exophytic if a cancer arises from the ectocervix, or may
be endophytic if it arises from the endocervical canal.
Mode of spread include direct extension , lymphatic
spread and hematogenous spread.
Histologic types are SCC(70%), adenocarcinoma (25%)
and other rare histologic types like mixed
adenosquamous , large cell neuroendocrine and small cell
neuroendocrine
48.
Diagnosis
In earlystage women diagnosed with this cancer are
asymptomatic.
In others, early-stage cervical cancer may create a watery
blood-tinged vaginal discharge.
Intermittent vaginal bleeding that follows coitus or douching
also can be noted.
occasionally, a woman presents with uncontrolled
hemorrhage from a tumor bed.
Other symptoms include chronic pelvic pain , loss of appetite
, weight loss and bowel and bladder symptoms
49.
Physical Examination
Mostwomen with this cancer have normal general physical
examination findings.
In those with suspected cervical cancer, a thorough external
genital and vagina examination is performed.
With speculum examination, the cervix can appear grossly
normal if cancer is micro invasive.
Visible disease displays varied appearances.
Lesions may be exophytic or endophytic growth; a polypoid
mass, or barrel-shaped cervix; a cervical ulceration or
granular mass; or necrotic tissue.
50.
During bimanualexamination, a clinician may palpate an
enlarged uterus resulting from tumor invasion and
growth , hematometra or pyometra.
With posterior spread. palpation of the rectovaginal
septum between the index and middle finger of an
examiner's hand reveals a thick, hard, irregular septum.
The proximal posterior vaginal wall is most commonly
invaded.
In addition, during digital rectal examination, parametrial,
uterosacral, and pelvic sidewall involvement can be
appreciated
Diagnostic workup
Biopsy preferablyby CKC or if not punch
biopsy
CBC,OFT,PICT
CXR
Abdominopelvic MRI
Cystescopy / proctoscopy /IVP based on
indication
53.
Staging
Historically, cervicalcancer has been staged clinically.
The current FIGO (2018)staging system now incorporates
radiologic and pathologic evaluation
Allowable components of clinical staging are
Cold-knife conization
Pelvic examination under anesthesia,
Cystoscopy, Proctoscopy,
Chest radiograph, and Intravenous Pyelogram (or this portion of
the computed tomography [CT] scan can be used).
See FIGO 2018 staging
54.
Management of cervicalcancer
1)Micro invasive diseases- option of treatment include
Cold knife conization(CKC)
Radical trachelectomy for those who want to preserve fertility
Simple extra facial hysterectomy
2)Early stage disease(IB-IIA)
One option for those with early stage diseases is RH+BPLND
For those who decline surgery or not fit for surgery ,primary chemo
radiation is other treatment option
3) Advanced stage diseases(stage IIB-IVA)
Primary chemo radiation is preferred treatment for this group of
patients
55.
4) Stage IVB
Patientswith stage IVB disease have a poor prognosis
and are treated with a goal of palliation.
Pelvic radiation is administered to control vaginal
bleeding and pain.
Systemic chemotherapy is offered to palliate
symptoms and prolong overall survival.
The chemotherapy regimens used in this group of
women are similar to those used in the setting of
recurrent cancer
56.
Surveillance
In general, patientsare seen at 3-month intervals for 2
years .
Then every 6 months until 5 years have passed from
treatment and then annually.
At each visit, in addition to pelvic examination, a
thorough manual nodal survey includes neck,
supraclavicular, axillary, and inguinal lymph nodes.
A cervical or vaginal cuff Pap test also is collected
annually for 20 years after treatment completion.
57.
Prognosis
FIGO stageis the most significant prognostic factor.
Lymph node involvement is an important prognostic feature,
and modified prognosis before it was formally incorporated
into the staging system.
For example, in early-stage cervical cancer (stages I through
IIA), nodal metastases are an independent predictor of survival.
In advanced- stage (stage IIB through IV) cervical cancer, lymph
node metastases also worsen prognosis.
In general, microscopic nodal involvement has a better
prognosis than macroscopic nodal disease.


![Staging
Historically, cervical cancer has been staged clinically.
The current FIGO (2018)staging system now incorporates
radiologic and pathologic evaluation
Allowable components of clinical staging are
Cold-knife conization
Pelvic examination under anesthesia,
Cystoscopy, Proctoscopy,
Chest radiograph, and Intravenous Pyelogram (or this portion of
the computed tomography [CT] scan can be used).
See FIGO 2018 staging](https://image.slidesharecdn.com/lectureoncervicalcaforc1-250217131012-0ca4f709/85/lecture-cervical-ca-note-for-year-three-medicine-students-53-320.jpg)
















































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)


















