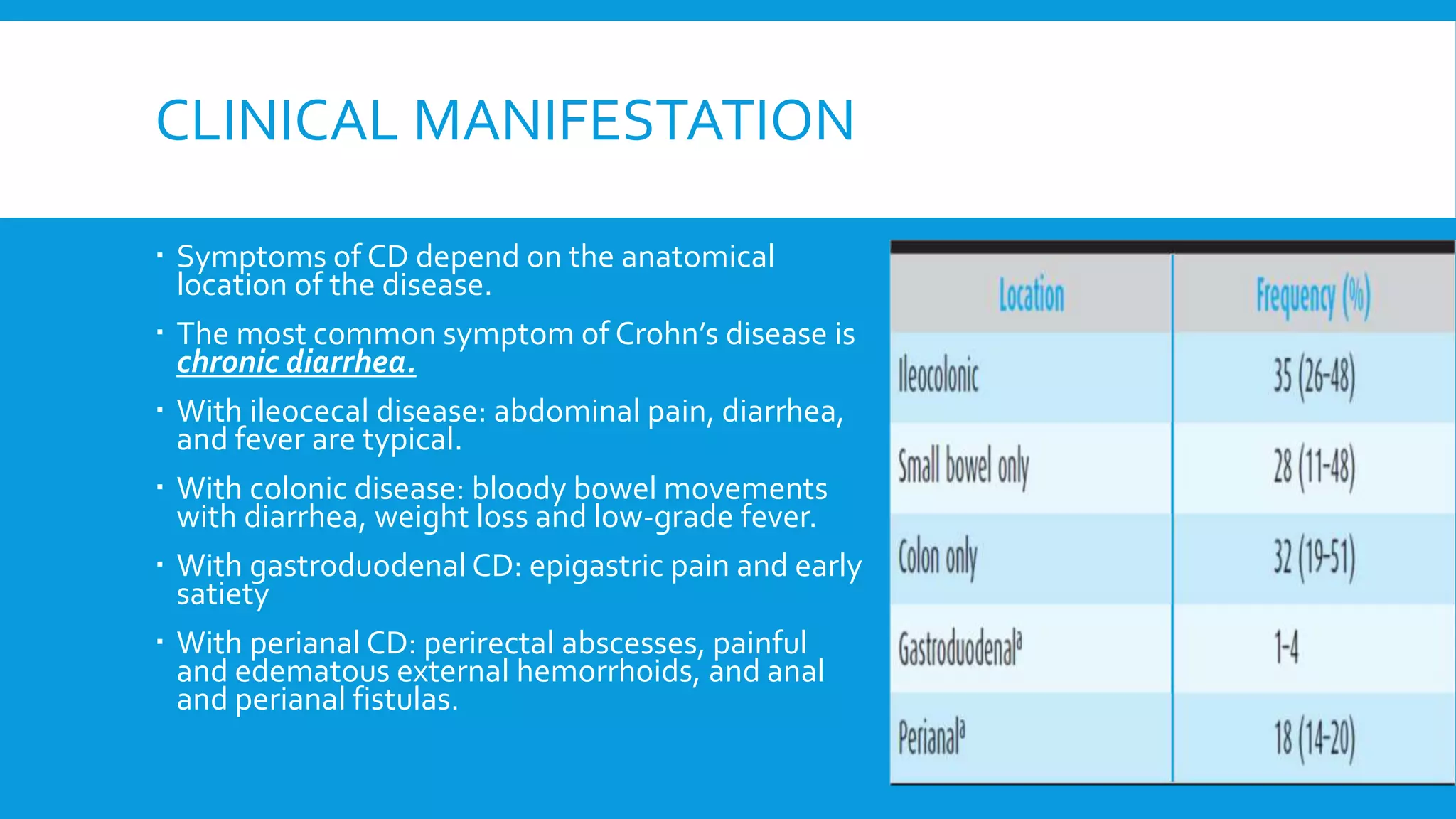
This document discusses the management of Crohn's disease in adults. It covers the clinical manifestations, natural history, prognostic factors, diagnosis, investigations including endoscopy and imaging, and medications used to treat mild to severe Crohn's disease. Treatment depends on the severity and location of inflammation, and may include mesalamine, corticosteroids, immunomodulators, anti-TNF agents, antibiotics, drainage of abscesses, and surgery. The goal of treatment is induction and maintenance of remission, and objective evaluation through endoscopy or imaging is important for monitoring disease activity over time.