Downloaded 48 times





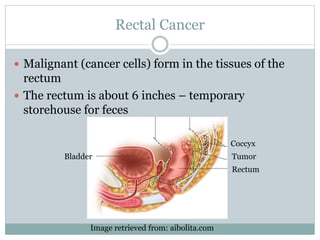
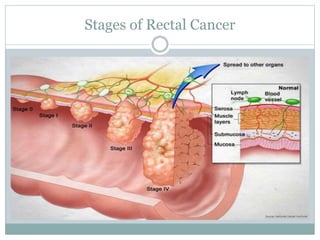



This webinar discusses rectal cancer. It begins with introducing the speaker and providing objectives for the webinar. It then covers topics such as prevalence and risk factors of rectal cancer, methods of diagnosis, determining the cancer stage, standard treatment options including surgery, radiation, chemotherapy and targeted therapy. Treatment is discussed in relation to cancer stage. The webinar also touches on survivorship issues and future research regarding rectal cancer.






































































































