Downloaded 412 times


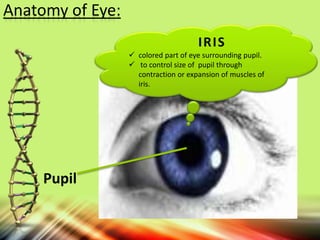
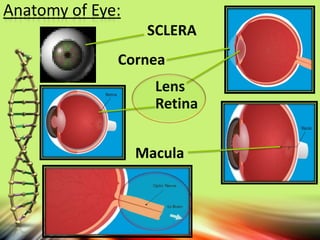
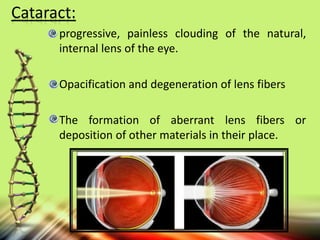


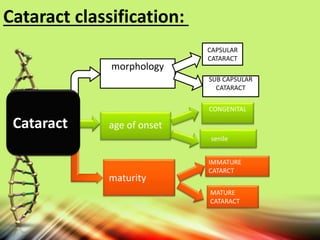
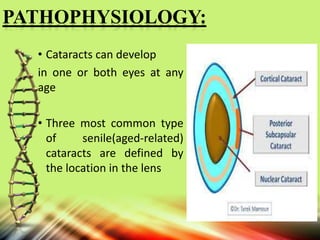

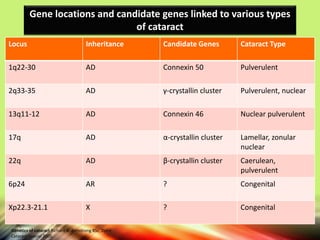
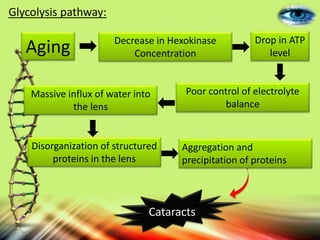
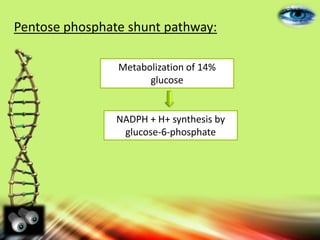
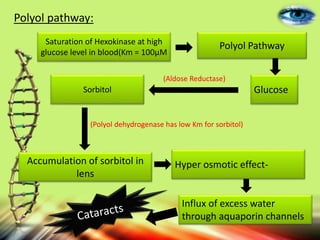
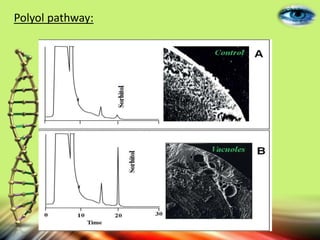



This document provides an overview of cataracts, including their anatomy, classification, pathophysiology, genetics, biochemical pathways, tests and treatments, prevalence, and references. It describes the key structures of the eye involved in cataracts such as the iris, pupil, sclera, cornea, and retina. It classifies cataracts based on location, age of onset, morphology, and maturity. The main pathophysiological mechanisms and risk factors are discussed. Genetic inheritance patterns and candidate genes are outlined. Biochemical pathways like glycolysis, the pentose phosphate shunt, and the polyol route are implicated in cataract formation. Tests, treatments, and prevalence statistics in Pakistan are summarized along with references



































































![Polymer [ बहुलक ] Chemistry Notes PDF - Irfanullah Mehar - JJ Sir Chemistry.pdf](https://cdn.slidesharecdn.com/ss_thumbnails/polymerchemistrynotespdf-irfanullahmehar-jjsirchemistry-260210172118-3f9b37f7-thumbnail.jpg?width=640&height=640&fit=bounds)







