Downloaded 52 times






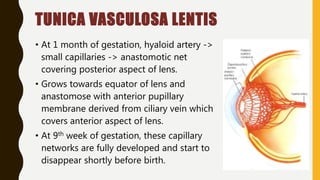












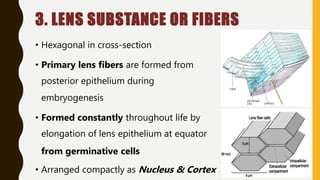

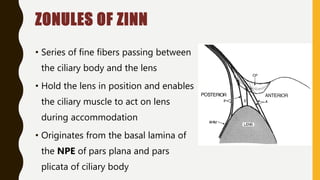










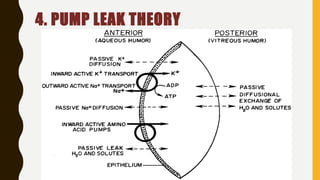




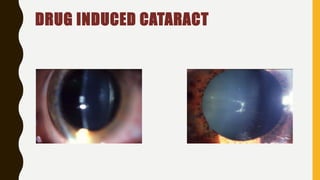



The document discusses the anatomy and physiology of the lens. It begins with the embryological development of the lens from surface ectoderm and describes the formation of the lens placode, pit, and vesicle. It details the anatomical structures of the lens including the capsule, epithelium, fibers, and zonules. The document also discusses the biochemical composition and metabolic processes that maintain lens transparency. Finally, it covers age-related changes to the lens and clinical significance including cataracts.



































































