Downloaded 45 times


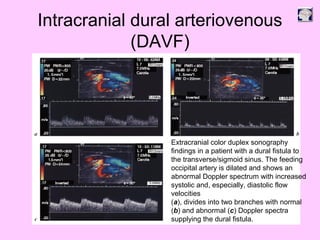
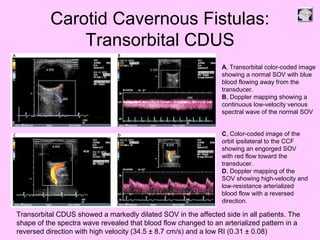
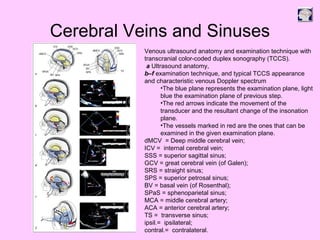
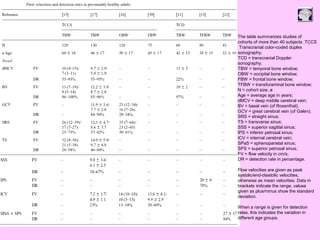
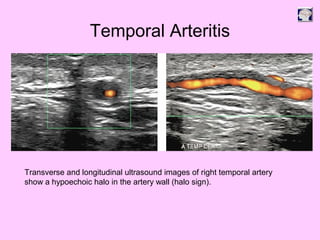
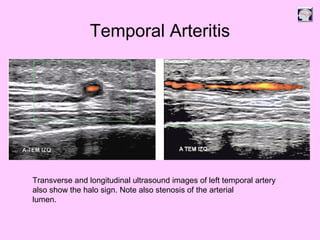
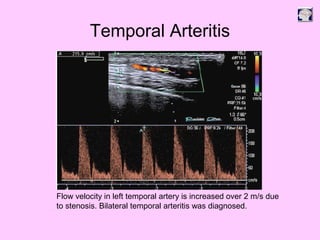
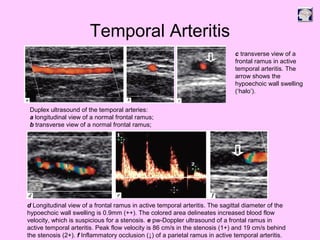


Ultrasound can be used to assess intracranial dural arteriovenous fistulas (DAVF) and carotid cavernous fistulas (CCF). For DAVF, ultrasound shows increased velocities in feeding arteries and decreased resistance indices, allowing assessment before and after treatment. For CCF, ultrasound reveals abnormal mosaic flow in the cavernous sinus and engorged veins with reversed flow. It can monitor hemodynamic changes and treatment response in a noninvasive manner. Ultrasound is also useful for assessing cerebral veins and sinuses, and can diagnose temporal arteritis by identifying hypoechoic wall thickening and stenoses in temporal arteries.





















































































