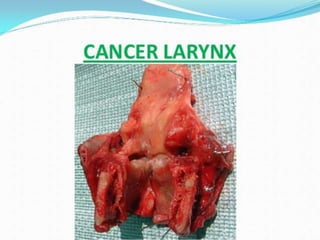
Laryngeal carcinoma is cancer that develops in the larynx (voice box). It is most commonly squamous cell carcinoma caused by risk factors like smoking, alcohol, asbestos, and chemicals. Symptoms include hoarseness, cough, throat pain, and lump in the neck. Diagnosis involves examination of the larynx and imaging tests. Treatment options include surgery to remove part or all of the larynx, radiation therapy, chemotherapy, and proton beam therapy. Nursing care focuses on airway clearance, pain management, nutrition, and communication strategies.
















































































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)









